Aiesha Ahmed1, William Jens1, Anne Haulman1, K. Sathian1, Stephen Ross1
Affiliation: 1Department of Neurology, Penn State Health, Hershey, PA, USA
Corresponding author: Aiesha Ahmed, aahmed1@ennstatehealth.psu.edu
Keywords: Cost-Effectiveness/Economic, Current Practice, eCONSULT, Electronic Medical Records, Models of Care, Neurological Care, Teleneurology Services, Blockchain, Fast Healthcare Interoperability Resources, FHIR, Interoperable data exchange, Voice biometrics
Section: Prespective, Opinion, and Commentary on a Current Issue Impacting the Sector
eConsults provide a mechanism for specialists to provide guidance to their colleagues to allow them to manage patients in primary care settings. The patient receives access to specialist expertise, avoids the long wait time and high costs associated with an office visit, and maintains relationship continuity with the primary care physician (PCP). The PCP has dynamic access to specialist expertise and an opportunity for attainting a higher comfort level with chronic neurological care comanagement. Patient referrals for specialty care are high, while there has been projected shortage in nonprimary care specialties.1,2 The increasing prevalence of neurologic diseases associated with an aging population will likely continue to increase the demand for neurologists.2,3
Electronic consultations (eConsults) are asynchronous provider-to-provider consultations (between aprimary care provider [PCP] and specialist) that occur within an electronic health record (EHR) or a web-based portal.4,5,6
The Association of American Medical Colleges (AAMC) formed a collaborative for implementation of an electronic medical record (EMR)-based, opt-in eConsult program across multiple academic medical centers (AMCs).7 The results at institutions participating in Project CORE (Coordinating Optimal Referral Experiences) include an 84% increase in timely access to specialty care and avoidance of an estimated 7,360 unneeded specialty referrals. As of 2018, the program has been implemented at 27 institutions where more than 2 million primary care patients can benefit from the model.8
Another example outside of Project CORE notes that eConsults for four specialties (dermatology, endocrinology, gastroenterology, and orthopedics) resulted in a reduction in face-to-face referrals and lower costs.9
To meet the neurological needs of patients referred by PCPs and other specialties, there is an opportunity for demand-shaping. The goal would be to increase or maintain the demand for early diagnosis and management of complex neurological diseases while decreasing the demand for ongoing care for chronic neurological conditions that can be provided by PCPs through collaboration, leading to decreases in fragmentation of care for the patients.
One way to approach this is to establish eConsult systems. The movement away from fee-for-service payment and toward value-based reimbursement and accountable care organizations creates incentives to improve patient care coordination.10 Even systems that support a fee-per-eConsult payment model may strongly consider developing this flexible care delivery model as there continues to be a transition to global payment models.4
The literature shows that benefits of eConsults outside of patient care included increasing PCP confidence/reassurance, gaining information on guidelines/literature/ resources, and acquisition of new knowledge.11
Neurology-specific eConsults offering has been explored by other countries successfully. The results highlight the benefits such as allowing prompt response to PCP inquires, early initiation of treatment, and reduced need for traditional visits to the clinics.12,13
Burnout is common in all neurology practice settings.14 Setting up eConsults provides another venue for addressing patient neurological care needs while providing flexibility and variety to the daily schedule of a specialist.
The following areas were explored to start our program.
The Chair and Clinical Vice Chair were onboard early on, which certainly helped our process. The faculty in neurology found the idea appealing, but questions were raised such as who would triage the queries; whether only general neurologists would participate, will there be protected time or assigned clinical full-time equivalent (FTE). From the referring physician side, we needed to identify champions who were either interested in piloting this with us or had been designated as the core group for Project CORE that our health system was to join (as the third cohort). This led to the next step of understanding and identifying the main players.
Stakeholders for eConsults are listed in Table 1.
Table 1. Stakeholders for eConsults
| Stakeholder | Rationale for inclusion in eConsults |
|---|---|
| Patients | At the center of this endeavor. |
| Providers (referring and consultants) | We believe that the neurologists will be comanaging patients with chronic neurological diseases in concert with PCPs, more so than before. Questions for ongoing care that can be addressed via eConsults will reduce the need for in-person visits, keep patients with a known/established provider, and decrease the burden of transportation/days off for caregivers to visit a specialty physician, in addition to timelier care of patients. We decided to launch our program with only the primary care group, with the goal to scale it up after this pilot. |
| Information technology (IT)/revenue cycle/legal | We engaged our IT colleagues to help with building the necessary templates in the EHR and the planning of future implementation of the billing component. Furthermore, we initiated ongoing discussion of patient consenting and of relevant legal considerations aspects that will need to be incorporated. Project CORE has been adding new AMCs over the years, which has provided precedents for this venture. Thus, healthcare systems can benefit (as we did) by reaching out to earlier cohorts of Project CORE participants to connect their IT, revenue cycle, and legal departments to initiate their eConsult programs. |
AMCs, academic medical centers; CORE, Coordinating Optimal Referral Experiences; EHR, electronic health record; PCPs, primary care physicians; IT, information technology.
With the shortage of neurologists nationally, we were concerned about launching this initiative on a large scale. We decided to start with general neurologists, and we have so far only engaged our two general neurologists for eConsults.
However, the discussion has been initiated for new faculty models to create teleneurology services (e.g., eConsult services, ambulatory teleneurology visits, inpatient teleneurology [stroke and nonstroke]), providing education/supervision to trainees). We believe that specific clinical FTE can be assigned to this role. Allowing current physicians to take on this role for a portion of their clinical effort can provide variety and work–life balance. The resulting experiences could blaze a trail for the department to establish new teleneurology services. This can potentially mitigate burnout and prepare us for finding new value care delivery models that may be geared toward population health.
We hope that over time, we would have at least one provider from each subspecialty available for participation. We also hope that exposing our trainees to this experience will broaden their horizons.
There are five components for establishing eConsults: templates, emergent care, establishing framework, billing codes, and relative value units (RVUs).
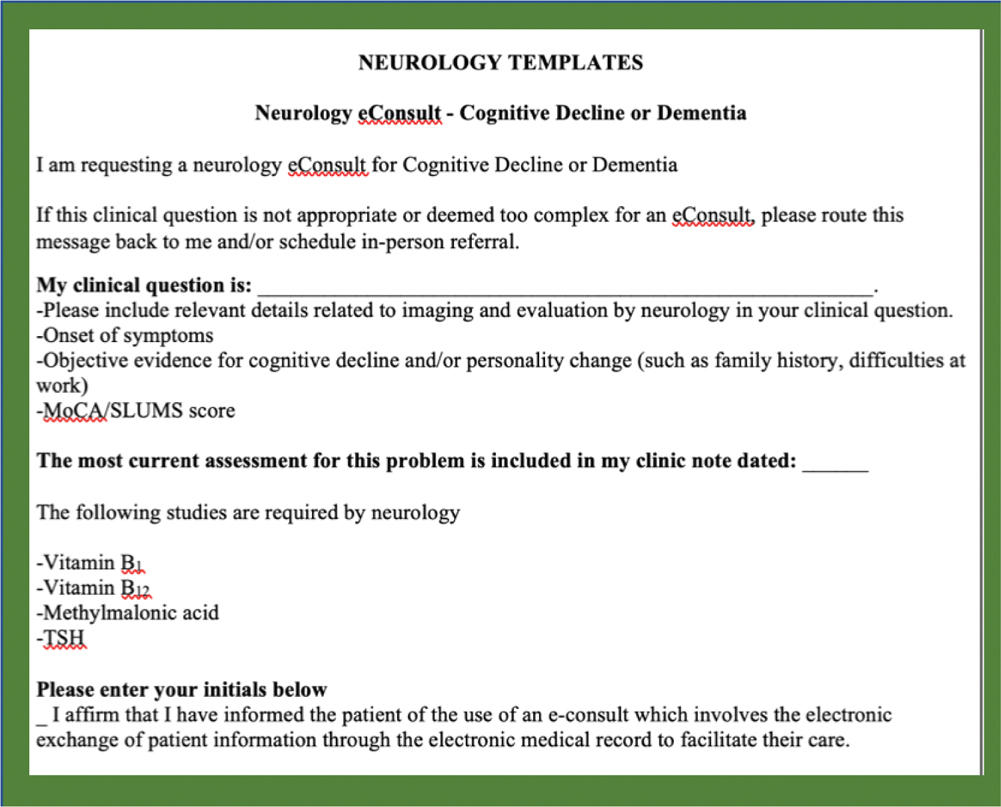
Templates. We launched with only 12 categories, to limit templates (Table 2). The format of these templates was created by reviewing examples from other institutions in earlier cohorts of Project CORE and discussion with our primary care colleagues (Figure 1).
Table 2. Twelve categories of eConsults
| Category | |
|---|---|
| 1 | Abnormal brain imaging |
| 2 | Tremors/abnormal movements |
| 3 | Cognitive decline |
| 4 | Dizziness/vertigo |
| 5 | Numbness, tingling/sensory loss |
| 6 | Headaches |
| 7 | Spells/seizures |
| 8 | Poststroke-related care |
| 9 | Gait disorder/parkinsonism |
| 10 | New abnormal laboratory or examination finding |
| 11 | Generalized weakness/fatigue |
| 12 | Unspecified |
Emergent care. Mutual agreement with referring providers established that eConsults are not to be used for urgent issues. These templates will not be used to send referrals for traditional clinic visits.
Figure 1—Neurology templates.
MoCA, Montreal Cognitive Assessment; SLUMS, Saint Louis University Mental Status; TSH, thyroid-stimulating hormone.
Establishing framework. Framework for the program included the following: (1) data collection to evaluate the time spent for each eConsult, (2) resource page creation on the intranet to share practice guidelines from appropriate professional organizations, such as the American Academy of Neurology (AAN), and (3) surveys to assess referring providers’ satisfaction.
Ultimately, we hope to quantitate demand relative to key symptoms or disorders. This will allow us to offer educational initiatives in those disease areas, and provide guidance toward hiring in and expansion of relevant subspecialty divisions.
Billing codes. On January 2019, new Current Procedural Terminology (CPT) codes, developed by the American Medical Association, were released that apply to bill eConsults for Medicare beneficiaries (Table 3). These codes are under review by our organization and have not yet been instituted.
Table 3. New CPT codes from January 2019
| CPT code | Description |
|---|---|
| 99451 | Interprofessional telephone/Internet/electronic health record assessment and management service provided by a consultative physician, including a written report to the patient’s treating/requesting physician or other qualified healthcare professional, 5 or more minutes of medical consultative time. |
| 99452 | Interprofessional telephone/Internet/electronic health record referral service(s) provided by a treating/requesting physician or qualified healthcare professional, 16–30 minutes.15 |
RVUs. The national payment rate will be approximately $37 for CPT code 99451 and CPT code 99452. This is determined based on 0.7 work RVUs, 0.29 practice expense RVUs, and 0.05 malpractice RVUs (the rate will vary by geographic region).15
We are allocating work RVU component in recognition of the time and effort of the neurologists performing eConsults. Even though billing for eConsults has not been instituted, the department and the institution view this venture as a step toward improving access by better serving the patients established with our primary care specialties while also addressing fragmentation of care. This also allows the neurologists involved to be more accessible to the PCPs electronically.
We recognize that to scale up eConsults requires a serious commitment by the departmental and institutional leadership. The commitment requires investment in a core implementation team, which includes an IT expert, a PCP champion and a specialist champion, development of fair reimbursement strategies for providers, and a commitment to system quality improvement.5
Our Neurology eConsult program is in its infancy. We hope to grow this offering and scale it up based on data we obtain from this pilot project.
We believe that eConsults provide another ramp onto the telehealth superhighway, to enable neurology practices to explore novel ways of coping with the national shortage of neurologists coupled with increased demand for access. eConsults offer one approach toward demand-shaping. This means that we can bring complex neurological patients to our attention sooner than is possible using the traditional consult system, by using eConsults to meet chronic neurological care needs of patients in a timely fashion through collaboration with primary care colleagues.
Conflict of Interest: Not applicable.
Contributors: All authors have contributed to the manuscript creation and to the project.
Funding Statement: Not applicable.
| 1. | Barnett ML, Song Z, Landon BE. Trends in physician referrals in the United States, 1999-2009. Arch Intern Med. 2012;172(2):163–70. https://doi.org/10.1001/archinternmed.2011.722 |
| 2. | Dall T, Chakrabarti R, Iacobucci W, Hansari A, West T. 2017 Update. The Complexities of Physician Supply and Demand: Projections from 2015 to 2030. Final Report. Association of American Medical Colleges. IHS Markit, Washington, DC. February 28, 2017. https://aamc-black.global.ssl.fastly.net/production/media/filer_public/a5/c3/a5c3d565-14ec-48fb-974b-99fafaeecb00/aamc_projections_update_2017.pdf |
| 3. | Dall T, Storm MV, Chakrabarti R, et al. Supply and demand analysis of the current and future US neurology workforce. Neurology. 2013;81(5):470–8. https://doi.org/10.1212/WNL.0b013e318294b1cf |
| 4. | Gleason N, Prasad PA, Ackerman S, et al. Adoption and impact of an eConsult system in a fee-for-service setting. Healthcare. 2017;5(1–2):40–5. https://doi.org10.1016/j.hjdsi.2016.05.005 |
| 5. | Tuot DS, Murphy EJ, Chen AH, et al. Evaluating diverse electronic consultation programs with a common framework. BMC Health Serv Res. 2018;18(1):1–11. https://doi.org/10.1186/s12913-018-3626-4 |
| 6. | Nuwer MR, Corboy JR. Clinical practice. Neurology. 2018;8(3):177–8. https://doi.org/10.1212/CPJ.0000000000000459 |
| 7. | Deeds SA, Dowdell KJ, Chew LD, Ackerman SL. Implementing an Opt-in eConsult Program at Seven Academic Medical Centers: a Qualitative Analysis of Primary Care Provider Experiences. JGen Intern Med. 2019;34(8):1427–1433. https://doi.org/10.1007/s11606-019-05067-7 |
| 8. | Available from: https://News.Aamc.Org/Patient-Care/Article/5-Ways-Econsults-Benefit-You-and-Your-Patients/ |
| 9. | Anderson D, Villagra VG, Coman E, Ahmed T, Porto A, Jepeal N, Maci G, Teevan B. Reduced Cost Of Specialty Care Using Electronic Consultations For Medicaid Patients. Health Aff (Millwood). 2018;37(12):2031–2036. https://doi.org/10.1377/hlthaff.2018.05124 |
| 10. | Schettini P, Shah KP, O’Leary CP, et al. Keeping care connected: e-Consultation program improves access to nephrology care. J Telemed Telecare. 2019;25(3):142–50. https://doi.org/10.1177/1357633X17748350 |
| 11. | Liddy C, Abu-Hijleh T, Joschko J, Archibald D, Keely E. eConsults and learning between primary care providers and specialists. Fam Med. 2019;51(7):567–73. https://doi.org/10.22454/FamMed.2019.407574 |
| 12. | Bradi AC, Sitwell L, Liddy C, Afkham A, Keely E. Ask a neurologist: What primary care providers ask, and reducing referrals through eConsults. Neurol Clin Pract. 2018;8(3):186–91. https://doi.org/10.1212/CPJ.0000000000000458 |
| 13. | Williams L, O’Riordan S, McGuigan C, Hutchinson M, Tubridy N. A web-based electronic neurology referral system: a solution for an overburdened healthcare system? Ir Med J. 2012;105(9):301–3. [cited 27 August 2019]. Available from: http://www.ncbi.nlm.nih.gov/pubmed/23240282 |
| 14. | Miyasaki JM, Rheaume C, Gulya L, et al. Qualitative study of burnout, career satisfaction, and well-being among US neurologists in 2016. Neurology. 2017;89(16):1730–8. https://doi.org/10.1212/WNL.0000000000004526 |
| 15. | Available from: https://www.aappublications.org/news/2019/01/04/coding010419 |
Copyright Ownership: This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, adapt, enhance this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0.