O. A. Burianov, Y. O. Yarmolyuk, T. M. Omelchenko, V.M. Lyanskorunsky, M. V. Vakulych
Affiliation: Bogomolets National Medical University
Corresponding Author: M. V. Vakulych, Email: vakulychmyroslav@gmail.com
Keywords: Fractures, Gunshot, Injury of Extremities, Long Bones, Quality of Care, Telemedicine, Trauma, Ukraine
Section: Original Clinical Research
Due to the armed conflict in the East of Ukraine, it is relevant to investigate factors that affect patient outcomes with the use of telemedicine. This applies especially to patients with multiple gunshot fractures, which is the most severe category at increased risk for complications and unsatisfactory results. A case study is reported here.
In the current combat conditions, 62.6% of injuries affect the extremities. Among these, reported injuries of the soft tissue account for 74.2% and fractures for 25.8% (of these, the percent of multiple injuries is 13.2%). In 49.4% cases of extremity injuries, fractures are accompanied by damage to the great vessels and nerves. Characterization of major complications include slow consolidation (81.2%) and pseudarthrosis (14.5%), osteomyelitis (18.1%), purulent-necrotic soft tissues (32.1%), and contractures of large joints (38.4%).1–7
The use of telemedicine in military conflicts during medical evacuation stages is documented.8,9 Due to the armed conflict in the East of Ukraine, it is relevant to investigate factors that affect patient outcomes—especially patients with multiple gunshot fractures—as this is the most severe group at increased risk for complications leading to unsatisfactory outcomes. Therefore, the goal of this article was to report on and contribute to the advancement of the rehabilitation treatment system for those with gunshot fractures of the long bones of the extremities.
Timely decision-making is one of the keys to improving the quality of care. The main complications affecting outcome in trauma patients include osteomyelitis, pseudo-arthrosis, and contractures of large joints. These complications develop over an extended period. Therefore, dynamic telemedicine monitoring is expected to help identify the signs of the above pathologies in a timely manner in order to minimize or prevent their development and progression.
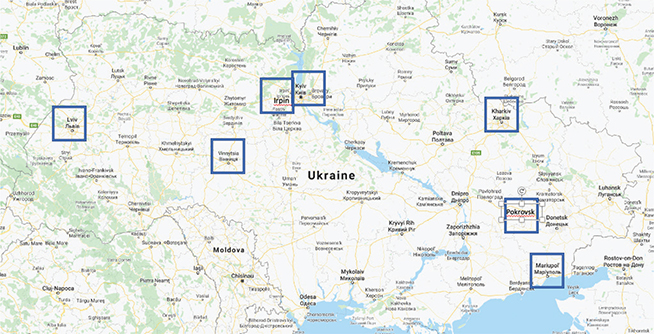
To ensure telemedicine system operation, medical evacuation levels were provided with technical and documentary equipment. From February 2015 to July 2017, a network of nine telemedicine centers was established, bringing together traumatology units of the National Military Medical Clinic (NMMC) Main Military Clinical Hospital (Kyiv); the Military Medical Clinical Centre (MMCC) for Occupational Pathology of the Personnel of the Armed Forces of Ukraine (Irpin); MMCC of Western Region (Lviv), Northern Region (Kharkiv), Southern Region (Odessa), and Central (Vinnytsia) Region; 66th Military Field Hospital (Pokrovsk); Bakhmut City Central District Hospital (CDH); and the 61st Military Field Hospital (Mariupol) (Figure 1).
Figure 1. A network of nine telemedicine centers in seven cities throughout Ukraine used for this project.
Computers, web cameras, televisions with High-Definition Multimedia Interface (HDMI) outputs, WIFI routers, high-speed Internet channels (100 Mbps), radiograph scanners, and Skype-telephony were used for the technical support of telemedicine technologies.
Patients and physicians signed informed consent to the teleconsultation (informed consent form approved at the meeting of the Committee on Bioethical Expertise and Ethics of Research at Bogomolets National Medical University [NMU], Kiev, Minutes No. 107 dated 29 December 2017).
Treatment was conducted in four stages corresponding to the levels of medical evacuation.
Following final osteosynthesis, the patient underwent a course of medical rehabilitation under individual rehabilitation program and osteoreparation monitoring (X-ray, multi-slice computed tomography), limb function recovery. If necessary, during rehabilitation, the patient could undergo stage surgical interventions (dynamics of fractures in case of blocking intramedullary rod osteosynthesis [nailing], fragmentary resection of fibular bone, tenolysis, myolysis, fistula sequester necrectomy).
The patient described below is characteristic of step-wise (routine/urgent) telemedicine consultations, “doctor–doctor” and “patient–doctor.” To evaluate the effectiveness of telemedicine consultations, telemedicine evaluation cards are pre-generated at Levels II, III, and IV of medical evacuation (teleconsultation at Level I medical evacuation is not available currently). The consulting institution is the traumatology department of NMMCC (National Military Medical Clinical Centre “Main Military Clinical Hospital,” Kyiv, Ukraine).
Patient B (age: 31 years) while in the military zone suffered a gunshot wound. Diagnosis was gunshot perforating injuries of the left thigh and lower leg with multiple fractures of the femur diaphysis in the lower third and diaphysis of the tibia in the middle third, with displacement of fragments.
Primary medical care was provided in the settings of the 66th Military Field Hospital (Pokrovsk) (primary surgical treatment, wound preservation, extrafocal osteosynthesis, aorto-enteric fistula of the femoral bone and tibia). A teleconsultation was held, and findings of pre-generated teleconsultation cards are shown in (Tables 1 and 2)
Table 1 Data and parameters of the telemedicine consultation results in a patient with multiple gunshot fractures of the long bones at Level II of medical evacuation*
| Data | Parameters | Results |
|---|---|---|
| Terms of telemedicine consultation | Routine (1) Urgent (3) |
3 |
| Clinical diagnosis | Confirmed (1) Clarified (2) Changed (3) |
2 |
| Clinical examination data | Confirmed (1) Clarified (2) Changed (3) |
2 |
| Data of laboratory tests performed (taking into account DCO) | Immediate correction required (3) No immediate correction required (1) |
3 |
| Laboratory Diagnostic Plan (taking into account DCO) | Confirmed (1) Clarified (2) Changed (3) |
1 |
| Imaging data | Immediate correction required (3) No immediate correction required (1) |
1 |
| Imaging diagnostic plan | Confirmed (1) Clarified (2) Changed (3) |
1 |
| Scope of surgical intervention (primary surgical treatment) | Complete (1) Not complete, routine correction (2) Not complete, urgent correction (3) |
2 |
| Does the patient require urgent surgery after teleconsultation? | Yes (3) No (1) |
3 |
| Disease management | Confirmed (1) Clarified (2) Changed (3) |
2 |
| Total | 20 |
*Patient B teleconsultation between the surgical department of 66th Military Field Hospital and the traumatology department of the National Military Medical Clinical Center.
DCO, Damage Control Orthopedics.
Table 2 Data and parameters of Patient B’s condition and scope of interventions according to Level II of medical evacuation*
| Data | Parameters | Results |
|---|---|---|
| Posttrauma admission time | Up to 6 hours (1) Up to a day (2) Up to 3 days (3) |
1 |
| Order of evacuation | First turn (3) Second turn (2) Third turn (1) |
2 |
| Multiple trauma type | Multiple (1) Combined (2) |
1 |
| Segment injury | Bilateral fractures of the lower extremities (2) Ipsilateral fractures of the lower extremities (1) Contralateral fractures of the lower extremities (2) Three lower extremity segments (3) Four lower extremity segments (5) Bilateral fractures of the upper extremities Ipsilateral fractures of the lower extremities Contralateral fractures of the lower extremities Three segments of the upper extremities Four segments of the upper extremities Multisegmented fractures of upper extremities + lower extremities − 2 seg. Multisegmented fractures of upper extremities + lower extremities − 3 seg. Multisegmented fractures of upper extremities + lower extremities − 4 seg. Multisegmented fractures of upper extremities + lower extremities − 5 seg. Multisegmented fractures of upper extremities + lower extremities − 6 seg. Multisegmented fractures of upper extremities + lower extremities − 7 seg. Multisegmented fractures of upper extremities + lower extremities − 8 seg. |
1 |
| Trauma severity according to PTS score | 10–19 score (3) 20–34 score (6) 34–48 score (8) 48+ (10) |
3 |
| Shock degree | None (1) I degree (2) II degree (4) III (6) IV (8) |
4 |
| Primary bone defect | Up to 3 cm (1) Up to 6 cm (3) Over 6 cm (5) |
3 |
| Great vessels damage | None (1) Present (4) |
1 |
| Fascial compartment pressure | Within normal (1) Mild local hypertensive ischemic syndrome (2) Moderate local hypertensive ischemic syndrome (3) Severe local hypertensive ischemic syndrome (4) |
3 |
| Transport immobilization at I level | Pneumatic splint (1) Cramer’s splint (2) Dietrich’s splint (3) |
2 |
| Level I wound healing | Performed (1) Not Performed (2) |
1 |
| Total | 22 |
*Patient B teleconsultation between the surgical department of the 66th Military Field Hospital and the traumatology department of the National Military Medical Clinical Center.
PTS, polytrauma score.
Telemedicine Consultation Efficiency Index based on the results (Table 1) is 2.0 (20 score/10 parameters = 2).The telemedicine consultation efficiency index for the conditions/interventions (Table 2) is 2.0 (22 score/11 parameters = 2).
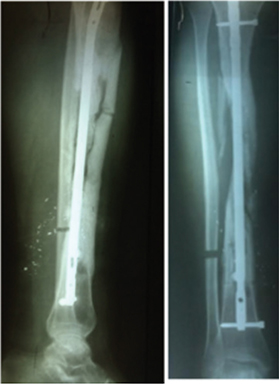
On the same day, the patient was evacuated to the MMCC of Northern Region (Kharkiv), where a “doctor–doctor” teleconference was held (Tables 3 and 4). Figure 2 shows X-rays of femur and tibia and a view of the lower extremity of Patient B during step-wise surgical treatments.
Table 3 Data and parameters of the telemedicine consultation results in patient with multiple gunshot fractures of the long bones at Level III medical evacuation*
| Data | Parameters | Results |
|---|---|---|
| Terms of telemedicine consultation | Routine (1) Urgent (3) |
3 |
| Clinical diagnosis | Confirmed (1) Clarified (2) Changed (3) |
1 |
| Clinical examination data | Confirmed (1) Clarified (2) Changed (3) |
1 |
| Data of laboratory tests performed (taking into account DCO) | Correction required (3) No correction required (1) |
3 |
| Laboratory diagnostic plan (taking into account DCO) | Confirmed (1) Clarified (2) Changed (3) |
2 |
| Imaging data | Correction required (3) No correction required (1) |
3 |
| Imaging diagnostic plan | Confirmed (1) Clarified (2) Changed (3) |
2 |
| Disease management | Confirmed (1) Clarified (2) Changed (3) |
3 |
| Did the telemedicine consultation change the surgical approach? | Yes (3) No (1) |
3 |
| Total | 21 |
*Patient B teleconsultation between the traumatology departments of the Military Medical Clinical Center of Northern Region (Kharkiv) and the National Military Medical Clinical Hospital.
DCO, Damage Control Orthopedics.
Table 4 Data and parameters of Patient B’s condition and scope of interventions according to Level III of medical evacuation*
| Data | Parameters | Results |
|---|---|---|
| Negative pressure therapy | Applied (1) Not applied (2) |
2 |
| Pulse-lavage | Applied (1) Not applied (2) |
2 |
| Fracture stabilization | Plaster immobilization (2) External fixation (1) |
2 |
| Need for reinstallation of external fixation device | Required (2) Not required (1) |
2 |
| Signs of segment inflammation | None (1) Present (2) |
2 |
| CFU (colony-forming unit) count | Less than 103 (1) 103–106 (2) More than 106 (4) |
4 |
| C-reactive protein | Within normal (up to 6 mmol/L) (1) 6–12 mmol/L (2) More than 12 mmol/L (4) |
4 |
| White blood cell count | Within normal (1) Leukocytosis (over 9 × 109)(3) |
3 |
| Hemoglobin | Within normal (1) Mild anemia (2) Moderate anemia (3) Severe anemia (4) |
3 |
| Albumen–globulin ratio | Within normal (1.5–2.3) (1) Lower 1.5 (4) Over 2.3 (2) |
4 |
| Ceruloplasmin | Within normal (20– 60 mg/dl) (1) Above normal (3) Below normal (2) |
3 |
| Total | 31 |
*Patient B teleconsultation between the traumatology departments of the Military Medical Clinical Center of Northern region (Kharkiv) and the National Military Medical Clinical Hospital.
Telemedicine Consultation Efficiency Index at Level III based on the results: 2.33 (21 score/9 parameters = 2.33) (Table 3).
Telemedicine Consultation Efficiency Index at Level III based on conditions and interventions: 2.8 (31 score/11 parameters = 2.8).
Figure 2. A. X-rays of femur and tibia. B. View of the lower extremity of Patient B during step-wise surgical treatments.
Following the teleconference, the patient received repeated surgical treatments using pulse lavage (Vol = 10 L NaCl 0.9%), tibia extrafocal osteosynthesis, apparatus of external fixation installation (additional rod installed of extrafocal fixator distal base of femur), transfusion with packed red cells (500 ml) and fresh frozen plasma (500 ml), identified C-Reactive Protein (CRP) (12 mmol/L), as well as ceruloplasmin (102 mg/dL), albumen–globulin ratio (1.3), hemoglobin after transfusion = 98 g/L; white blood cell (WBC) count = 13.2 × 109 CFU was not determined until the next teleconsultation in 2 days, which established: telemedicine consultation efficiency index at Level III based on results = 1.22. The telemedicine consultation efficiency index at Level III based on the conditions/interventions = 2.09.
Due to the patient’s stable condition, he was transferred to the Traumatology Department, Clinic of Injuries, NMMC. The following procedures performed in NMMCC included stage-wise surgical treatments using negative pressure therapy technology, ultrasonic cavitation. A cement spacer with antibiotic (vancomycin) was installed in the area of tibia tissue defect, wounds suture (CFU Staphylococcus aureus 103 prior suturing).
Eleven days later, due to the absence of signs of inflammation and wound healing, the sutures were removed, and laboratory and instrumental examinations were performed: WBC = 8.4×109/L; CRP = 8.9 mmol/L; ceruloplasmin 52.4 mg/L; albumen–globulin ratio = 1.6; hemoglobin = 112 g/L. Doppler ultrasonography did not reveal signs of phlebothrombosis of both lower extremities.
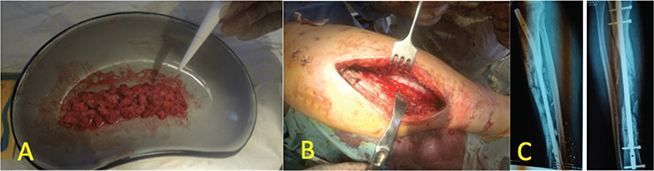
Due to the satisfactory course of the wound, with absence of inflammation, it was decided to perform convert fixation, with the following surgical intervention: sampling of spongy bone tissue from both wings of the iliac bones, spongy-fibrinous autoplasty of tibial defect, blocking intramedullary rod osteosynthesis of the left tibia, and blocking intramedullary rod osteosynthesis of the left femur. The findings are shown in Figure 3.
Figure 3. A. Spongy bone tissue with platelet-rich fibrant sealant; B. Appearance of defect of the tibia bone after sponge-fibrin autoplasty; C. Lower leg X-rays of Patient B after nailing, sponge-fibrin autoplasty.
The postoperative period was unremarkable. Therefore, 8 days after surgery, the patient was transferred to the Military Hospital in Irpin for step-wise rehabilitation. The following teleconsultation took place 2 weeks after the start of rehabilitation in Irpin Military Hospital (Tables 5–7).
Table 5 Data and parameters of telemedicine consultation for patient with multiple gunshot fractures of long bones at Level IV medical evacuation (specialized treatment + rehabilitation centers)*
| Data | Parameters | Results |
|---|---|---|
| Terms of telemedicine consultation | Routine (1) Urgent (3) |
1 |
| Clinical diagnosis | Confirmed (1) Clarified (2) Changed (3) |
1 |
| Clinical examination data | Confirmed (1) Clarified (2) Changed (3) |
1 |
| Data of laboratory tests performed | Correction required (3) No correction required (1) |
1 |
| Laboratory diagnostic plan | Confirmed (1) Clarified (2) Changed (3) |
1 |
| Imaging data | Correction required (3) No correction required (1) |
1 |
| Imaging diagnostic plan | Confirmed (1) Clarified (2) Changed (3) |
1 |
| Disease management | Confirmed (1) Clarified (2) Changed (3) |
2 |
| Rehabilitation potential | Method conversion step (0) Confirmed (1) Requires confirmation (2) |
1 |
| Total | 10 |
*Patient B teleconsultation between the traumatology departments of the Military Hospital (Irpin) and the National Military Medical Clinical Hospital. Telemedicine Consultation Efficiency Index at Level IV based on scope of interventions: 1.11 (10 score/9 parameters = 1.11) (0 results not taken into account).
Table 6 Data and parameters of the patient’s condition and scope of interventions according to Level IV medical evacuation (specialized treatment)*
| Data | Parameters | Results |
|---|---|---|
| Negative pressure therapy | Applied (1) Not applied (2) Wound healed (0) |
0 |
| Pulse lavage | Applied (1) Not applied (2) Wound healed (0) |
0 |
| Fracture stabilization | Plaster immobilization (2) Apparatus of external fixation (1) Method conversion performed (0) |
0 |
| Need for AEF reinstallation | Required (2) Not required (1) Method conversion performed (0) |
0 |
| Signs of segment inflammation | None (1) Present (2) |
1 |
| Colony-forming units | Less than 103 (1) 103–106 (2) More than 106 (4) Wound healed (0) |
0 |
| C-reactive protein | Normal range (up to 6 mmol/L) (1) 6–12 mmol/L (2) Over 12 mmol/L (3) |
2 |
| WBC count | Normal range (1) Leukocytosis (more than 9 × 109) (3) |
1 |
| Hemoglobin | Normal range (1) Mild anemia (2) Moderate anemia (3) Severe anemia (4) |
2 |
| Albumen–globulin ratio | Normal range (1.5–2.3) (1) Lower 1.5 (4) Over 2.3 (2) |
1 |
| Ceruloplasmin | Normal range (20–60 mg/dl) (1) Above normal (3) Below normal (2) |
1 |
| Method conversion | Performed (1) Not performed (3) |
1 |
| Spacers | Applied (1) Not applied (2) No defect (0) |
1 |
| Total | 10 |
*Patient B teleconsultation between the traumatology departments of the Military Hospital (Irpin) and the National Military Medical Clinical Hospital. Telemedicine Consultation Efficiency Index based on main values at Level IV (Irpin—NMMCC): 1.5. (18 score/12 parameters = 1.5) (0 results not taken into account).
AEF, apparatus of external fixation; WBC, white blood cell.
Table 7 Data and parameters of telemedicine consultation for patient with multiple gunshot fractures of long bones at Level IV medical evacuation (rehabilitation centers and outpatient) and outpatient treatment
| Procedure | Findings | Results |
|---|---|---|
| Fracture consolidation | In line with terms (1) Delayed consolidation (2) |
1 |
| Fracture dynamization (after nailing) | Required (2) Not required (1) No nailing applied (0) |
1 |
| Fractional resection of fibular bone | Required (2) Not required (1) Other segment (0) |
1 |
| Need for reapplication of regenerative technologies | Required (2) Not required (1) |
2 |
| Correspondence of function (movement amplitude) with the postoperative period | Required (2) Not required (1) |
1 |
| Regeneration technologies | PRP (1) PRF (1) Not applied (2) |
1 |
| Range of motion in the joints of the injured extremities | Within normal (1) Mild (2) Moderate (3) Severe (4) |
3 |
| Purulent complications | None (1) Soft tissue (2) Osteomyelitis (3) |
1 |
| Pain syndrome | Trend to lower (1) Unchanged (2) Increased pain syndrome (3) |
1 |
| Segment shortening | None (1) Up to 2 cm (2) More than 2 cm (3) |
1 |
| Muscle hypotrophy | None (1) Up to 2 cm (2) More than 2 cm (3) |
3 |
| Vascular disorders | None (1) Lymphostasis (2) Phlebotrombosis (3) |
2 |
| Total | 18 |
PRF, platelet-rich fibrin; PRP, platelet-rich plasma.
Following teleconsultation, the patient was discharged to continue treatment as an outpatient under the supervision of a traumatologist and was granted medical leave. “Doctor–patient” teleconsultations were held every 2 weeks, and a satisfactory course of treatment was established. Eleven weeks after surgery, the patient requested a remote examination. Inflammation was observed in the area of the distal part of the left lower leg (distal locking screw), and the patient had fever (maximum up to 37.8°C) with increased pain.
As additional examination was required, the patient was referred to MMCC of the Northern Region (Kharkiv), where, following laboratory-instrumental examination, “doctor–doctor” telemedicine consultation was held. Laboratory test results were as follows: WBC = 10.8 × 109/L, CRP = 11.4 mmol/L, ceruloplasmin = 62.7 mg/L, albumen–globulin ratio = 1.5, hemoglobin = 118 g/L. It was determined that in the area of the distal blocking screw, there was a functioning fistula. X-ray revealed fibular bone consolidation, an unsatisfactory course of tibia consolidation (lack of signs of developing primary osteotylus). It was decided to remove the screw and perform fistula necrectomy and fibular bone resection (Figure 4). Telemedicine consultation efficiency index was based on integrative values at Level IV: 2.33 (28 score/12 parameters = 2.33) (0 results are not taken into account) (Table 7); telemedicine consultation efficiency index was based on results = 2.8 (Table 5).
Figure 4. Lower leg X-rays of Patient B after fragmentary fibular bone resection with screw removal (due to the presence of fistula and its migration).
Subsequently, the patient was referred again to Irpin Military Hospital for the course of rehabilitation treatment. Any complications occurred after further routine teleconsultations. After 1 year of treatment, the patient was treated in NMMCC. At the request of the patient, the nail was removed.After wound healing, the patient was examined (Figures 5 and 6).
Figure 5. Functional treatment outcome in Patient B 12 months after last surgery.
Figure 6. X-ray of femur and tibia in Patient B 12 months after last surgery.
The Mattis–Luboshutz–Schwartzberg scale, a modification of Shevtsov, was used to evaluate the long-term treatment outcome. In this scale, we mark the results of every patient on 10 parameters: pain, range of motion (joint), segment shortening, deformation, lameness, muscle hypotrophy, vascular and neurological disorders, infectious complications, and efficiency, and the following was established: absence of pain syndrome; a slight restriction in motion (extensor contracture of the knee joint with slight impairment of function); limb shortening by 1 cm; no deformity of the limb; no vascular, neurological, or purulent complications; presence of muscle hypotrophy (hip 1 cm, lower leg 0.5 cm); slight lameness; recovery of work capacity (patient returned to duty). The score is 36, the average score is 3.6 (10 criteria).
The algorithm for decision-making was based on the pre-determined system that exists in Ukraine for the treatment of patients with multiple gunshot fractures. According to this concept, at each stage, the main criteria and indicators are defined, making it possible to move to the next stage. Each card (described in detail below) corresponds to the level (role) of medical care in Ukraine, where each parameter receives points. Greater significance of a parameter (severity of condition, critical situation, etc.) results in a higher score.
Each teleconsultation card has a maximum number of points. For example, data and parameters of the patient’s condition and scope of interventions, according to Level II of medical evacuation, have a maximum score of 49. The patient with this result will be at maximum severity and require the maximum number of interventions.
It should be noted that because of the results of our previous studies (unpublished), there was no situation when, during a certain consultation, the patient was evaluated at a minimum scale on almost every score, or on one or two parameters at the maximum. For example, there were no previous patients with segment injury (ipsilateral fractures of the lower extremities [one point]), trauma severity (posttraumatic score of 10–19 [three points], great vessels damage (none [one point], and maximum score of shock degree (IV [eight points]).
It should be noted that the weight assigned to each indicator differs. “Shock degree,” for example, is much more important than the parameter, “Transport immobilization at I level,” and the score assigned is higher.
The following scheme is proposed for the evaluation of the consultation score, with the maximum score at each stage divided into three degrees of severity.
Respectively, there are three degrees of severity that define the patient’s condition. In addition, there are three degrees of effectiveness of teleconsultation (because, at each stage, two cards were evaluated: the main indicators of the patient’s condition and treatment tactics after teleconsultation.) Conventionally, these are low, medium, and high levels of consultation effectiveness, and mild, moderate, and severe levels of the patient’s condition.
In Table 3, data and parameters of telemedicine consultation results in Patient B, with multiple gunshot fractures of the long bones at Level III medical evacuation teleconsultation between traumatology departments of the Military Medical Clinical Center of Northern region (Kharkiv), and National Military Medical Clinical Hospital), and Table 4.
Data and parameters of the patient’s condition and scope of interventions according to Level III of medical evacuation for Patient B (based on teleconsultation between the traumatology departments of the Military Medical Clinical Center of the Northern region (Kharkiv) and the National Military Medical Clinical Hospital—a teleconsilium—and the patient’s condition) were performed immediately after the patient’s admission, with the level of performed interventions estimated at 31 points (index 2.8) (with a maximum score of 32, and a maximum index of 2.9), that is, a Telemedicine Consultation Efficiency Index at Level III based on the “results” of 2.33 (21 score/9 parameters), with a maximum of 27 points and a maximum index of 3.0). Thus, the patient’s condition was rated as “severe” and the effectiveness of consultation was “high.”
Discussed and implemented treatment tactics were effective as assessed at the next consultation (after 2 days), with telemedicine consultation efficiency index at Level III based on results = 1.22 (with a maximum of 3.0). The telemedicine consultation efficiency at Level III was based on “conditions and interventions” at 2.09 (23 points out of a maximum of 31). That is, teleconsultation was no longer so effective, the patient’s condition had improved, but, of course, during the 2 days that passed between the consultations, the laboratory parameters could not become normal (as a result of gunshot polytrauma). Such a patient was considered to be of moderate severity and did not require surgery, only intensive (infusion therapy, etc.) treatment.
Due to the fact that patients with multiple long bone fractures are at an increased risk of complications (e.g. osteomyelitis, delayed consolidation/pseudarthrosis, contractures of the large joints), the option considered to improve the rehabilitation treatment outcome included telemedicine consultations. No similar methodology is found in the literature to evaluate the effect of teleconsultations on the clinical outcome.
This clinical case is an example of employing telemedicine to guide the treatment of a patient with trauma related to multiple gunshots. Teleconsultation cards were generated to monitor the examination effectiveness. In this case, it was noted that teleconcilium at Level II medical care resulted in changes to treatment requiring urgent surgery. At the outpatient stage of treatment, the diagnosis and treatment of implant-associated infectious complications were performed in a timely manner. Timely decision-making and complete implementation of rehabilitation treatment system resulted in a good outcome.
Telemedicine consultations at the level of medical evacuation can affect the rate of decision-making in the treatment of patients with multiple gunshot fractures of the long bones.
In the future, it is planned to compare and conduct a prospective randomized trial, with the goal of predicting treatment outcomes depending on teleconsultation assessments (based on integrative values and results). Using appropriate statistical analysis, the prognostic effect of a telemedicine consultation will be determined based on the effectiveness of the results of the treatment of injured patients using functional scores, incidence of developing osteomyelitis, pseudarthrosis, and contractures of large joints.
Funding statement: None
Conflict of interest: None
Contributors: Each author contributed to the writing, editing, and data assessment reported in the article.
| 1. | Abakumov MM, Lebedev NV, Malyarchuk VI. An objective assessment of the severity of injury in patients with combined injuries. Bull Surg. 2001;160(6):42–5. |
| 2. | Ankin N. Politrauma (organizational, tactical and methodological problems). Medpress-inform; 2004: 176 p. |
| 3. | Buriyanov OA, Laksha AM, Yarmolyuk YO. Modern aspects of recovery treatment of patients with multiply gunshot fractures. Traumatol Orthop. 2013;(3–4):94–8. |
| 4. | Buriyanov OA, Laksha AM, Savka IS, et al. Primary surgical treatment of patients with gunshot injuries. Ukrainian Medical Newsletter. Therapy. 2014;10(92):42–4. |
| 5. | Buriyanov OA, Laksha AM, Savka IS, et al. Principles of primary surgical care of victims with gunshot limb fractures. Modern aspects of military medicine: Collection of scientific articles of the Main Military Medical Clinical Center. 2014;21:393–400. |
| 6. | Buriyanov OA, Laksha AM, Yarmolyuk YO, Laksha AA. Step-wise surgical treatment of patients with gunshot fractures. A list of traumatology and orthopedics. 2015;1–2(31–32):50–3. |
| 7. | Zarutsky YL, Aslanyan SA, Shudrak AA. Guidance of military surgery. Kyiv: Department of the Ministry of Defense of Ukraine; 2014: p.400. |
| 8. | Nettesheim N, Powell D, Vasios W, et al. Telemedical support for military medicine. Mil Med. 2018;183(11–12):e462–70. https://doi.org/10.1093/milmed/usy127 |
| 9. | Weymouth W, Thaut L, Olson N. Point of view telemedicine at point of care. Cureus. 2018;10(11):e3662. https://doi.org/10.7759/cureus.3662 |