Ishaan Rischie, BA, Biosciences;1 Athena Walker, MS;2 Eduardo Garcia, MS;2 Robert Oru, MS;2 Sweta Sneha PhD3
Affiliations: 1Kinesiology, and Medical Humanities Minor, Rice University (Houston, TX, USA); 2Healthcare Management and Informatics, Kennesaw State University (Kennesaw, GA, USA); 3Professor and Executive Director, Healthcare Management and Informatics, Kennesaw State University (Kennesaw, GA, USA)
Corresponding Author: Sweta Sneha, ssneha@kennesaw.edu
Keywords: COPD, Data Analytics, Medicare, Readmission, Telemedicine
Section: Original Clinical Research
Objective: Telemedicine has developed as an innovative way to remotely view and treat patients without necessitating for patients to physically come into a physicians’ office or healthcare facility. This study aims to provide insights into the effectiveness of integrating telemedicine in medical facilities, where patients have high hierarchical condition category (HCC) risk scores.
Design: This study utilized two raw datasets: (1) a Centers for Medicare & Medicaid Services (CMS) dataset created from the 2017 Medicare Physician and Other Supplier National Provider Identity Aggregate Report and (2) a National Center for Education Statistics (NCES) dataset created from the NCES table on the number and percentage of households in each state with computer and internet access. A regression analysis was carried out on the CMS dataset to determine the correlation between HCC risk scores and the reimbursement lost by healthcare facilities, where over 50% of their patients are diagnosed with chronic obstructive pulmonary disease (COPD). A second analysis was conducted with the NCES dataset to show which states had a high proportion of both households with internet access and COPD patients. A final regression analysis was run and translated into an interactive map in order to determine which regions of the United States could most benefit from telemedicine adoption.
Results: This study discovered a number of physicians and healthcare facilities in the eastern region of the United States that could benefit significantly from telemedicine applications. These findings were supported by the locations and data abstracted from facilities with high numbers of COPD patients, which were found to have poor HCC risk scores and thus high reimbursement losses.
Conclusions: This study confirmed the association between HCC risk scores and reimbursement losses. In order to alleviate those losses, this study identified states across the United States that should choose to incorporate telemedicine into how they diagnose and treat patients based on the needs of healthcare facilities and the internet capabilities of households in those states, because telemedicine integration presents the potential to improve patient HCC risk scores and reimbursement amounts by lowering readmission rates while also promoting higher patient and physician satisfaction. Future efforts should develop specific strategies to assist with telemedicine implementation and should track the observed effects of its adoption on reimbursements and quality of care.
The hierarchical condition category (HCC) risk score is a system implemented by the Centers of Medicaid and Medicare Services (CMS) to determine patients’ future medical needs in a medical coding format according to diagnoses and diagnostic coding (ICD-9-CM).1 Chronically ill patients receive a HCC risk score as an assessment of the amount of reimbursement a healthcare facility could expect to profit or lose.2 Provision of reimbursements to healthcare facilities depends on proper determination of HCC risk scores by taking a number of different variables into account, including different patient diagnoses and their likelihood of readmittance. Accurate patient diagnostic coding is especially necessary for those patients who suffer from other diseases in addition to their chronic illness. Misdiagnosing or underdiagnosing a patient who suffers from multiple comorbidities can result in inaccurate HCC risk scores and greater losses for the facility.2
Because the CMS-HCC model is typically used for chronic illnesses, this study focuses on chronic obstructive pulmonary disease (COPD), one of the most widespread chronic diseases worldwide with at least 16 million people living with COPD in the United States alone.3 COPD is one of the leading causes of death in the United States, causing over 150,000 deaths each year.3,4 According to the CMS, patients hospitalized for COPD have a 30-day readmission rate of 22.6. Given the high burden of readmission in addition to the already staggering number of existing cases, COPD was added to the Medicare Hospital Readmission Reductions Program, in 2015, resulting in financial penalties for COPD readmissions within 30 days of hospital discharge.5
Hospitals or healthcare facilities responsible for treating patients with chronic illnesses like COPD that has to be readmitted on a consistent basis are likely to have worsening HCC risk scores, which can prove detrimental not only to the quality of care but also to the amount of reimbursement a facility.6 Since the beginning of Medicare’s implementation of the HCC risk score, there has been a direct correlation between the risk score factor and reimbursement rates for facilities.7 After examining how hospital finances affect the quality of care they deliver, Akinleye et al.8 concluded that there is a strong positive correlation between performance scores and reimbursement amounts and hospital performance scores and reimbursement amounts, and a strong negative correlation between performance scores and readmission rates. There is an abundance of existing literature that provides evidence in support of this assertion that financially unstable, low-revenue, or low-reimbursement healthcare facilities and hospital systems are less capable of reliably providing high-quality care.9–12
Nevertheless, ensuring that patients who receive the best care possible should always be a top priority for healthcare providers. When high-quality health care is administered to patients, their overall quality of health improves as well as their general satisfaction with their doctor or physician.8,13 This is where telemedicine comes in. With the staggering number of COPD cases each year, it would be beneficial for facilities treating COPD patients to incorporate telemedicine into their treatment options. If physicians were able to give round-the-clock care to COPD patients, they could better detect sudden changes or declines in health.7,14–15 By bringing clinical care to patients at home, telemedicine enables healthcare practitioners to reduce the long-term risk of patients and make personalized adjustments, which would ultimately reduce the need for patients to frequently visit doctors’ offices and hospitals and lead to a subsequent decrease in their readmission rates in these facilities. In fact, there has been a consistent, strong parallel between the adoption of telemedicine practices in healthcare facilities and the reduction of readmission rates since its first introduction to society in the late 1950s and early 1960s.16 O’Connor et al. found that telemedicine and telehealth were shown to cause a 73% relative reduction in the readmission rates for a Medicare-certified home healthcare agency over the course of 3 years.17 Consequently, reduced readmissions as a result of telemedicine integration is likely to reduce HCC risk scores of patients.
The adoption of telemedicine practices and methods in healthcare facilities could have positive effects on readmission rates, facility reimbursement amounts, and overall satisfaction with quality of care for both patients and providers. Despite these positive effects, telemedicine adoption faces several obstacles to implementation. Ronda et al.18 concluded that unawareness is the primary barrier to enrollment in a virtual telemedicine platform designed to connect physicians with patients with diabetes mellitus, another chronic disease. For uninformed or untrained patients, the ability to talk with their providers face to face without physically being in a doctor’s office may seem counterintuitive. Thus, one of the most crucial steps toward getting providers and patients to begin incorporating telemedicine into their practices is providing patients with detailed knowledge about telemedicine platforms, thereby helping patients recognize and understand the potential benefits. Kruse et al.19 published a systematic review in 2018, in which several patient barriers hindering telemedicine adoption were identified, including the most salient patient barriers being the age, level of education, eHealth or computer literacy, unawareness, and bandwidth of dwelling. Collectively, these barriers similarly suggest a general lack of patient awareness and education about telehealth advances. In addition, Kruse et al. point to the need for a certain degree of internet access and computer literacy in order to successfully implement telemedicine and reap its benefits.
This study aims to provide a systematic analysis on the ways in which the HCC risk score affects reimbursement rates for healthcare facilities where half or more of the patients seen suffer from COPD. In addition, this analysis will identify the regions of the United States which contain healthcare facilities and households that are likely to benefit the most from telemedicine. In addition, this analysis will provide novel insights into the effectiveness of integrating telemedicine with standard practices in these medical facilities as a measure to reduce their readmission rates, which, in turn, will improve HCC risk scores as well as facility payout rates.
This literature review led to the establishment of the following analytic inquiries: (1) how medical facilities are affected by their insurance revenue, (2) how HCC risk scores are correlated with reimbursement amounts, (3) how telemedicine is known to reduce the amount of readmissions for healthcare facilities, and (4) how telemedicine can reduce the overall HCC risk scores. In order to address these queries, several different statistical analyzations were carried out on two different datasets containing raw data. The first dataset from the CMS—Medicare Physician and Other Supplier National Provider Identifier (NPI) Aggregate Report, Calendar Year 2017—contains a number of different variables, including utilization, payments (Medicare allowed amount, Medicare payment, standardized Medicare payment), and submitted charges organized by NPI along with demographic information for each facility listed and their corresponding HCC risk score.20 A subset of this data was created to identify those healthcare facilities, where over 50% of the patients treated at that facility were diagnosed with COPD. This data subset was used to show the correlation between the HCC risk score and Medicare reimbursement amount, as well as a correlation to show which providers and facilities across the United States would benefit the most from the integration of telemedicine according to their HCC risk score. The second dataset from the NCES—Table 702.60.Number and percentage of households with computer and internet access, by state—includes all households whose members access the Internet at home by paying a cell phone company or internet service provider.21 This dataset was used to show how many households across the United States have access to internet capabilities as a proxy measure for the ability to utilize telemedicine practices. Both the article reviews and the data analysis complement each other as each article referenced in the research shows a direct correlation to the specific analyses ran using the raw data.
The first analysis was a regression analysis, calculated using the subset of the first dataset—Medicare Physician and Other Supplier NPI Aggregate Report, Calendar Year 2017—to show the correlation between HCC risk score and the reimbursement amount for healthcare facilities, where over 50% of their patients are diagnosed with CPD. In order to obtain data for patients who were specifically suffering from COPD, the dataset was filtered by the variable “Provider Type,” explicitly selecting providers that specialize in pulmonary disease. The filtered dataset was then uploaded into the programing system SAS Studio, where the regression analysis was run to evaluate whether HCC score has an impact on the reimbursement amount not paid for COPD patients. The dataset contained 10,000 different variables for HCC score, so it was necessary to group each of the HCC risk scores by state before performing the regression analysis in order to properly calculate and compare the correlations between HCC risk score and amount of reimbursement. This method was supported by Yeatts and Sangvai1 since the “CMS-HCC risk-adjustment model was designed to most accurately predict spending at the group level, not the individual beneficiary level. Thus, the expenditure predicted for an individual beneficiary is likely to be less accurate than the expenditure predicted for a group of beneficiaries.” After the dataset was filtered and grouped accordingly, the analysis was conducted.
The second analysis was done using a dataset from the NCES—Table 702.60.Number and percentage of households with computer and internet access, by state: 2016—to show the average number of households across the United States with internet accessibility, therefore showing which states could viably adapt to telemedicine. Because the correlation of the initial dataset from CMS was done for Medicare patients, the focus of the second dataset was on patients in the oldest age group (50+). This age group was chosen because it is most inclusive of the desired population COPD is typically diagnosed in patients older than 45 years of age, and most elder patients will qualify for Medicare as an insurance once they reach 65 years of age.22 There was no need for this data to be filtered since the dataset did not contain an overly large or abnormal amount of data, so it was uploaded directly into the programing application Microsoft Azure, where several graphical analyses were run to determine which households in the United States have the highest internet access.
A final analysis was then run using an SAS linear regression model of the CMS data subset to show which regions of the United States have healthcare facilities that would most benefit from the adoption of telemedicine methods based upon their HCC risk score and Medicare reimbursement amounts. This final regression analysis was translated into an interactive map.
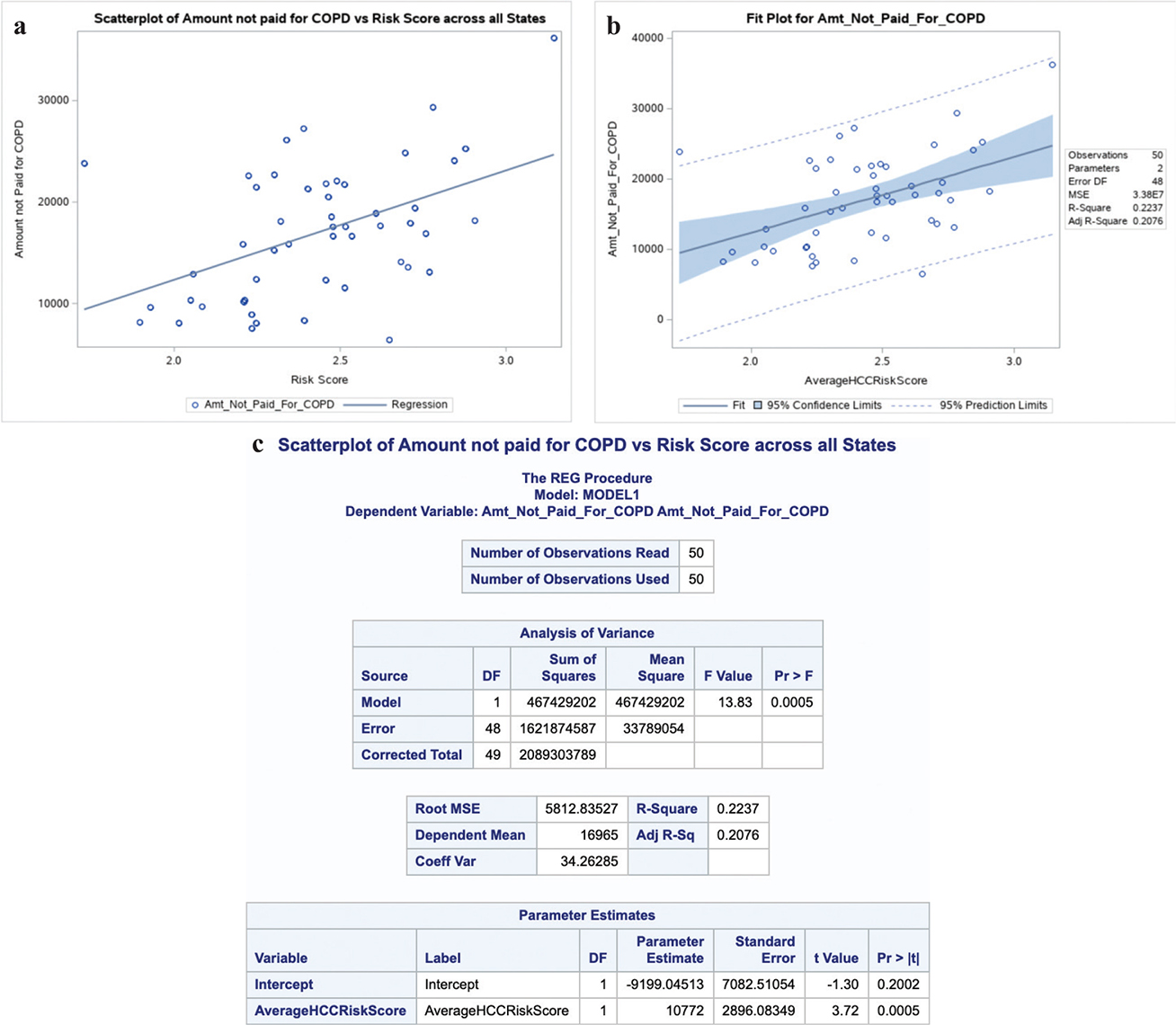
The regression analysis ran on the CMS dataset was plotted into a scatterplot to show the correlation between the average HCC risk score and the reimbursement amounts not paid to each one of the healthcare facilities, representing their reimbursement losses (Figure 1A). The analysis showed a moderate positive relationship between the dependent and independent variables with a correlation coefficient of r = 0.47 (Figure 1C). This scatterplot demonstrates that as the HCC risk score increases (based upon the average risk scores for each of the 50 states), the amount of reimbursement lost by hospitals and facilities increases as well. Along with the correlation coefficient, an R-squared value of 0.2237 was found, indicating that 22.37% of the variation in the reimbursement amount not paid for COPD patients was due to a variation in the HCC risk scores. Furthermore, the amount not paid for COPD patients increased by approximately $10,772 on average, per point increase in HCC risk score, shown by the “Parameter Estimates” listed in the regression analysis for the average HCC risk scores by state (Figure 1C). An additional fit plot (Figure 1B) was created to depict the scatterplot of the regression analysis along with the regression line, prediction interval, and confidence interval. The confidence interval makes an estimate for the average individual with a particular HCC risk score. The prediction interval is wider to account for the risk in trying to make a prediction for an individual.
Figure 1—Regression analysis of CMS dataset showing the positive correlation between HCC risk scores and the Medicare reimbursement amount for healthcare facilities. (A) Scatterplot of HCC risk score versus amount not paid for COPD patients. (B) Fit plot of the data along with the regression line, prediction interval (indicated by dashed lines), and confidence interval (indicated by solid blue region). (C) Regression analysis statistics.
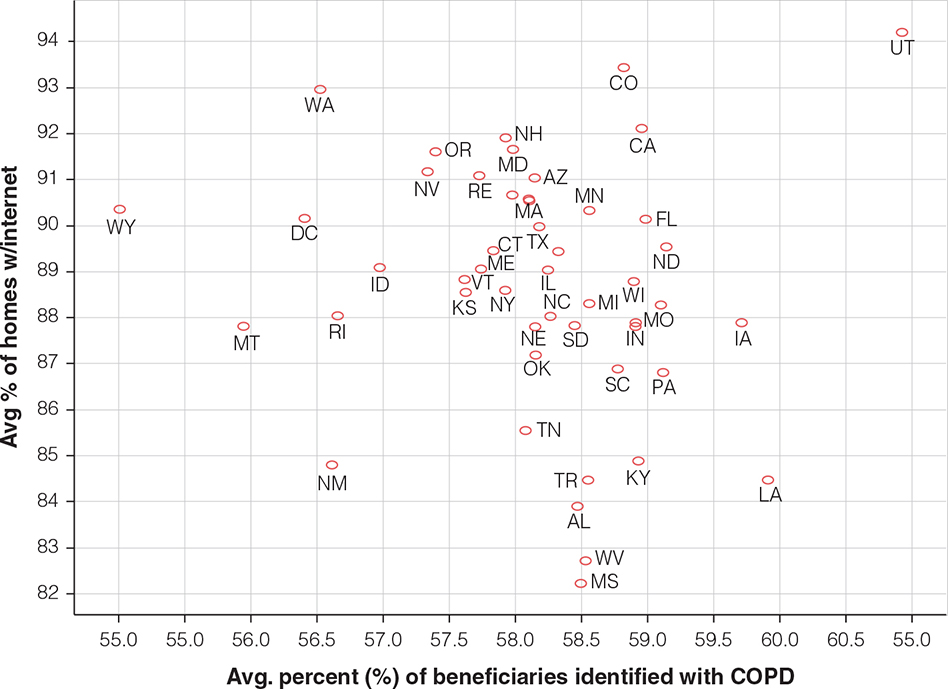
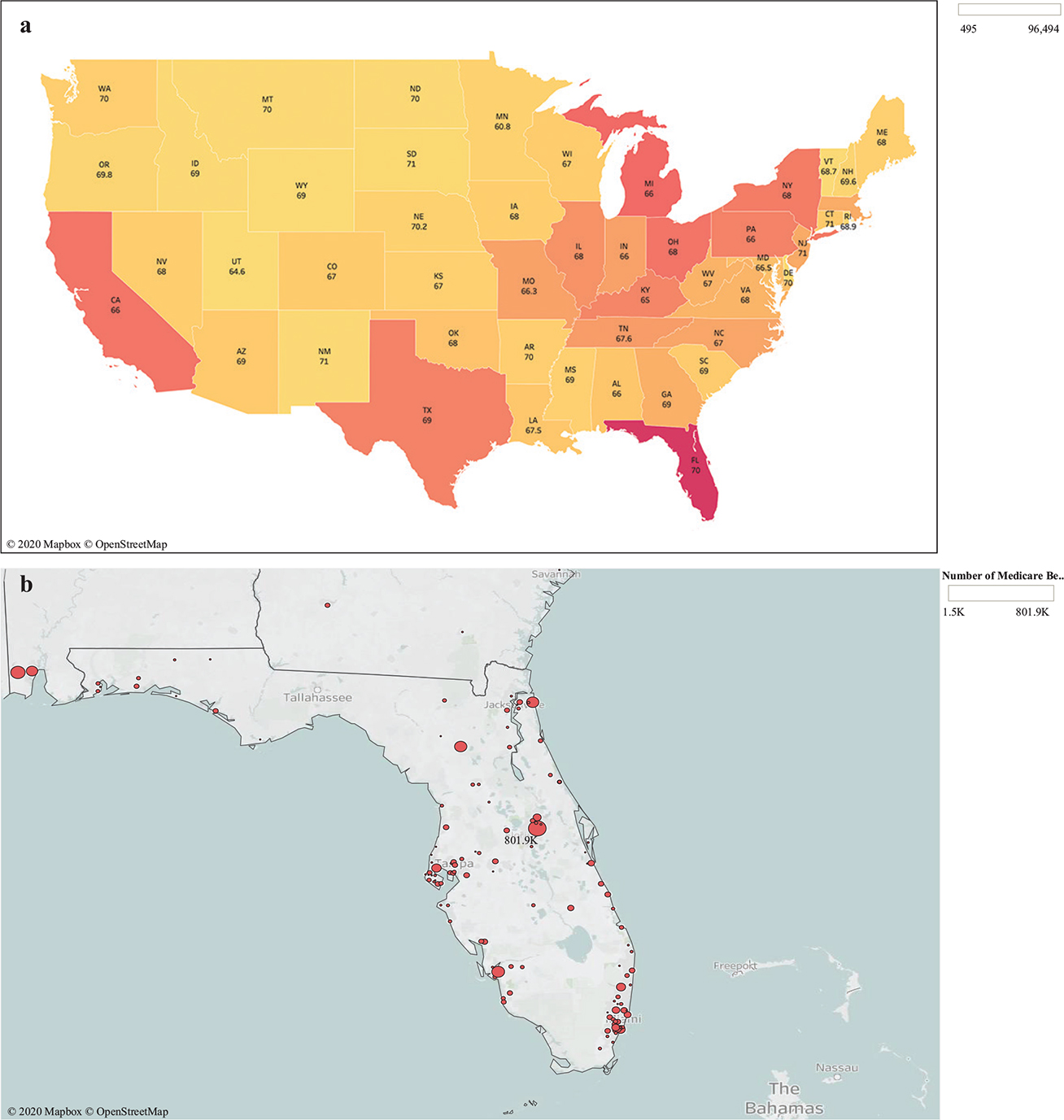
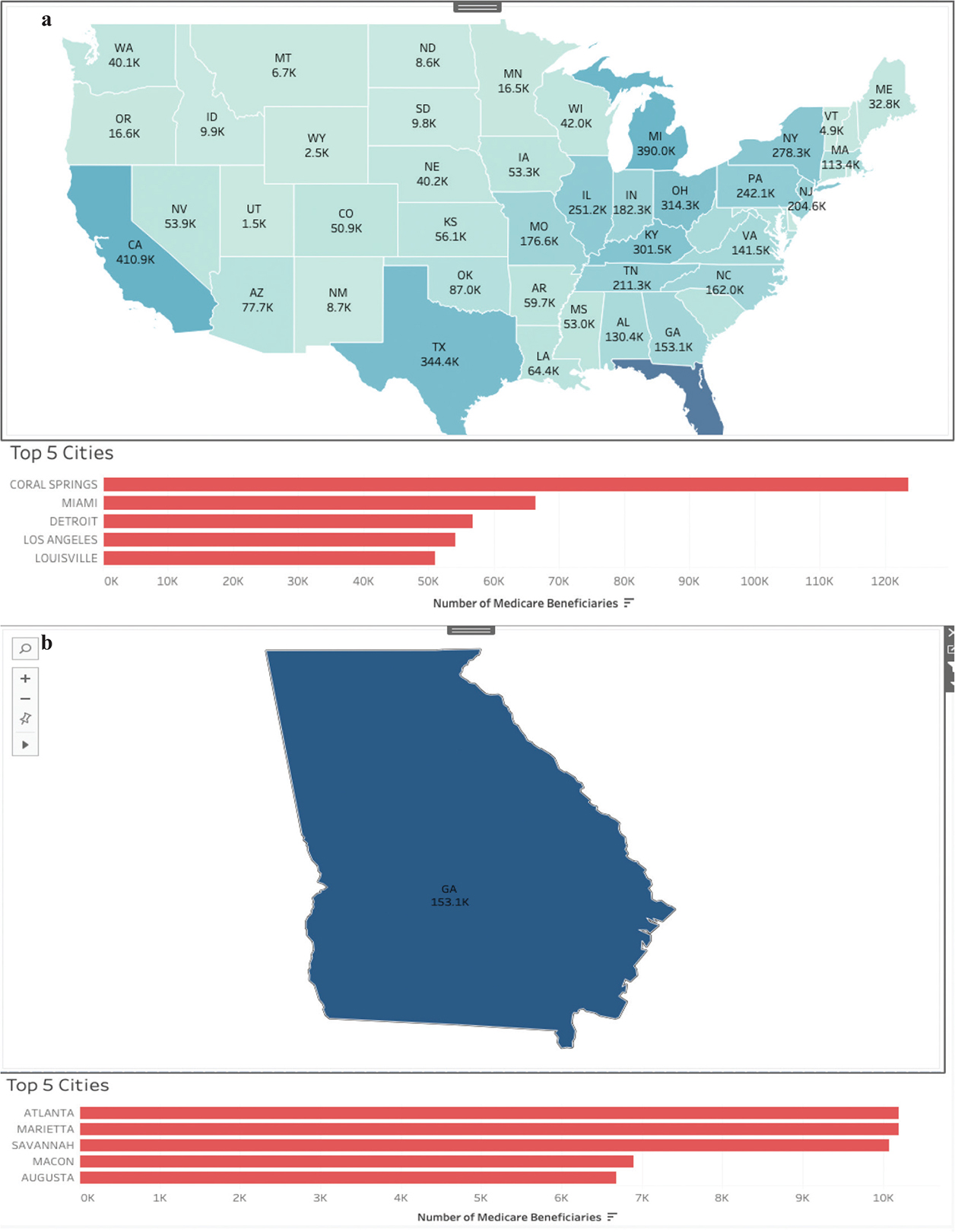
Using the dataset from the NCES, this study found the number of households in the United States that are capable of utilizing their home internet for telemedicine. Figure 2 shows a scatterplot for the association between states and the percentage of households with internet access. Analysis of this scatterplot revealed a much higher portion of states on the eastern half of the United States with homes with internet access than the north western half of the country. This analysis was also done in combination with the graphical analysis in Figure 3A, which shows the percentage of patients with COPD across the United States. By accounting for both the percentage of patients with COPD and the number of households with access to the internet, the state-level analysis suggests that California, Florida, Michigan, Kentucky, Ohio, New York, and Pennsylvania would benefit the most from telemedicine. The state with the highest percentage of COPD patients and the highest percentage of patients with access to internet was Florida (Figure 3B). Based on the CMS data, an interactive mapping guide was designed with a drill-down analysis of the overall map of the United States (including state and city levels) to show the percentages of patients who have been identified with COPD (Figure 4).
Figure 2—Graphical analysis of the numbers of households across the United States with access to the Internet.
Figure 3—Saturation of COPD Medicare beneficiaries by state. (A) In the nation-level map, yellow states show states with the lowest percentage of patients with COPD, while red states show the highest percentage of COPD patients. The average age of the COPD Medicare beneficiaries is listed below each state abbreviation. (B) Florida, the state with the highest amount of COPD patients who will benefit from telemedicine.
Figure 4—Examples of interactive mapping guides created (A) for the entire United States and (B) for a single state, which, in this case, is Georgia.
Based upon the regression analysis of the CMS raw dataset, our findings did demonstrate that the HCC risk score is associated with the amount of reimbursement that medical facilities and hospitals receive. The regression analysis proposes a moderate positive correlation between the HCC risk score and the amount of reimbursement loss. This finding is consistent with the existing body of scientific works, which en masse maintains that as the risk score increases, the amount of money that medical facilities will lose.7 In other words, a higher HCC risk score would denote a larger amount of money lost from the reimbursement. Because Medicare accounts for two different variables when calculating the risk score, the HCCs may be assumed to have a direct correlation to both the amount of times a patient is readmitted and the patient’s particular diagnosis. This finding is particularly significant for healthcare facilities that treat chronic conditions like COPD, which is associated with abnormally high readmission rates, as these hospital systems may begin struggling with financial upkeep as a result of the low reimbursements. Financial stability in healthcare facilities is a well-documented precursor for diminishments in the overall quality of care and performance ratings.9
The adoption of telemedicine has been known to produce improvements in patient readmission rates. Reducing readmission rates with telemedicine can continuously improve HCC risk scores over long periods of time. Because our analysis shows a direct correlation between the HCC risk scores and the amount of money a healthcare facility loses in reimbursements, telemedicine-induced improvements in readmission rates and HCC risk scores could reduce the amount of reimbursements lost by healthcare facilities. According to our analyses, states on the east coast of the United States along with California are likely to benefit the most from telemedicine adoption as these states tend to be the most saturated with COPD patients and to have the most homes with internet access. Florida appears to be the state with the highest amount of COPD patients and households with internet accessibility. Therefore, because COPD patients are more likely to be given high HCC risk scores, healthcare facilities in Florida would be expected to reap greater benefits than most other states by adopting telemedicine practices for patients diagnosed with COPD. Nonetheless, all of the identified states—Florida, California, Michigan, Kentucky, Ohio, New York, and Pennsylvania—have the technological capabilities and the COPD burden to significantly benefit from integrating healthcare facilities with telemedicine practices in the treatment of COPD and other chronic illnesses.
The regression analysis performed on the raw data from the CMS plotted a weak correlation between the HCC score and reimbursement amounts per patient. This could be attributed to grouping the HCC risk scores by state when determining the correlation between HCC risk scores and amount of reimbursement lost. Though an earlier regression was carried out where each patient was accounted for individually, the analysis was incomprehensible due to the large dataset of over 10,000 patients. Upon further research, this study confirmed that, not grouping together, the HCC risk factors by state or other variables in addition to the COPD variable could show an imprecise correlation, which is why the presented regression analysis was conducted by grouping-related HCC risk factors.1 The filters placed on the second dataset from the NCES constitute a potential limitation as well. Though the initial dataset was quite large, filtering it by both age and provider type may have made the study population less representative of all COPD patients (from the CMS dataset) and all households (from the NCES dataset) across the United States. If an accurate or large enough sample was not evaluated, there is a possibility that the observed conclusions drawn from each of the analyzed populations could lack external validity.
The goal of this study was to investigate how the HCC risk scores model has an effect on the amount of reimbursement that healthcare systems are paid by Medicare. This analysis confirmed that the HCC risk score does in fact have a direct correlation with Medicare reimbursement amounts for facilities, as well as with the readmission rates for patients. It was also shown that the enactment and maintenance of telemedicine and telehealth practices can reduce readmissions for patients, which will concurrently reduce patients’ HCC risk scores as well. The regression analysis for the correlation between HCC risk score and Medicare reimbursement lost was shown to have a positive correlation when calculated. In combination, all of the findings concurred that there are relevant associations between HCC risk scores, readmissions, and medical facility reimbursements. Our second analysis identified regions across the United States that would benefit the most from telemedicine usage. Locations were selected based upon the number of households in the United States with internet access and the healthcare facilities in the United States that commonly treat COPD patients (these facilities would thus have the highest amount of reimbursement lost based on the HCC scores of the COPD patients). This analysis showed that the Eastern half of the United States (with the exception of California) contains the highest proportion of facilities that would benefit the most, with Florida having the highest percentage of COPD patients and the highest number of households with access to internet. The span and implications of this research could be expanded in future research efforts by not limiting the provider type to pulmonary physicians in order to investigate all providers that treat patients with Medicare. This method would provide a larger sample size to represent a larger collection of the Medicare population. Furthermore, in order to see an increase in patients’ health and a reduction in HCC risk scores, future efforts should develop specific strategies to implement telemedicine practices in healthcare facilities in the states identified in this research. Following implementation, a large-scale analysis of the observed effect telemedicine adoption in these facilities that correlate to physician reimbursements from Medicare would prove useful. If successful telemedicine implementation shows an association with increased reimbursements and quality of care, the collective research could support how value-based care, continuous care, and preventative care methods have a strong impact on facility reimbursement rates.
Conflicts of interest: The authors declare no conflicts of interest.
Contributors: SS made substantial contributions to the conception, design, and supervision of the work; AW, EG, and RO contributed to data acquisition, cleansing, and analysis; IR, AW, EG, and RO contributed to the interpretation of data for the research. IR made critical and extensive contribution to drafting the research for publication. IR, AW, EG, RO, and SS contributed to reviewing and/or revising the draft for critical intellectual content. IR, AW, EG, RO, and SS contributed to the final approval of the research for publication. IR, AW, EG, RO, and SS are in agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding statement: Not applicable.
| 1. | Yeatts JP, Sangvai DG. HCC coding, risk adjustment, physician income: What you need to know. Fam Pract Manag. 2016[cited];0900:24–7. Available from: https://www.aafp.org/fpm/2016/0900/p24.pdf |
| 2. | Mehta HB, Dimoouo F, Adhikari D, et al. Comparison of comorbidity scores in predicting surgical outcomes. Med Care. 2016[cited];54(2):180–7. https://doi.org/10.1097/MLR.0000000000000465 |
| 3. | NIH. NIH statement on World COPD Day 2018. 2018 [cited 2020 June 29]. Available from: https://www.nih.gov/news-events/news-releases/nih-statement-world-copd-day-2018 |
| 4. | Omachi TA, Gregorich SE, Eisner MD, et al. Risk adjustment for health care financing in chronic disease: What are we missing by failing to account for disease severity? Med Care. 2013[cited];51(8):740–7. https://doi.org/10.1097/MLR.0b013e318298082f |
| 5. | Portillo EC, Wilcox A, Seckel E, et al. Reducing COPD readmission rates: Using a COPD care service during care transitions. Fed Pract. 2018[cited];35(11):30–6. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6366592/ |
| 6. | Turcotte J, Samford Z, Broda A, Patton C. Centers for Medicare and Medicaid Services Hierarchical Condition Category score as a predictor of readmission and reoperation following elective inpatient spin surgery. J Neurosurg Spine. 2019[cited];31(4):600–6. https://doi.org/10.3171/2019.3.SPINE1999 |
| 7. | Health Catalyst Editors. Five action items to improve HCC coding accuracy and risk adjustment with analytics. Health Catalyst; 2019 [cited 2020 June 29]. Available from: https://www.healthcatalyst.com/insights/5-ways-improve-hcc-coding-accuracy-risk-adjustment |
| 8. | Akinleye DD, McNutt L, Lazariu V, McLaughlin CC. Correlation between hospital finances and quality and safety of patient care. PLoS One. 2019[cited];14(8):e0219124. https://doi.org/10.1371/journal.pone.0219124 |
| 9. | Bazzoli GJ, Clement JP, Lindrooth RC, et al. Hospital financial condition and operational decisions related to the quality of hospital care. Med Care Res Rev. 2007[cited];64(2):148–68. https://doi.org/10.1177/1077558706298289 |
| 10. | Encinosa WE, Bernard DM. Hospital finances and patient safety outcomes. Inquiry. 2005[cited];42(1):60–72. https://doi.org/10.5034/inquiryjrnl_42.1.60 |
| 11. | Dong GN. Performing well in financial management and quality of care: Evidence from hospital process measures for treatment of cardiovascular disease. BMC Health Serv Res. 2015[cited];15:45 https://doi.org/10.1186/s12913-015-0690-x |
| 12. | Smith RB, Dynan L, Fairbrother G, Chabi G, Simpson L. Medicaid, hospital financial stress, and the incidence of adverse medical events for children. Health Serv Res. 2012[cited];47(4):1621–41. https://doi.org/10.1111/j.1475-6773.2012.01385.x |
| 13. | Prakash B. Patient satisfaction. J Cutan Aesthet Surg. 2010[cited];3(3):151–5. https://doi.org/10.4103/0974-2077.74491 |
| 14. | Wicklund E. Using telemedicine to boost HEDIS, reduce risk and fight blindness. mHealth Intelligence; 2016 [cited 2020 June 29]. Available from: https://mhealthintelligence.com/news/using-telemedicine-to-boost-hedis-reduce-risk-and-fight-blindness |
| 15. | Baggot D, Glick S, Lapsley H, Garg P, Javanmardian M, Macphearson M. Telehealth’s opportunities in new Medicare advantage rule. Oliver Wymman; 2019 [cited 2020 June 29]. Available from: https://health.oliverwyman.com/2019/04/cms-permits-telehealth-coverage-for-rural-medicare-patients.html |
| 16. | History of telemedicine. md Portal, September 23, 2015 [cited 2020 June 29]. Available from: http://mdportal.com/education/history-of-telemedicine/ |
| 17. | O’Connor M, Asdornwised U, Dempsey ML, et al. Using telehealth to reduce all-cause 30-day hospital readmissions among heart failure patients receiving skilled home health services. Appl Clin Inform. 2016[cited];7(2):238–47. https://doi.org/10.4338/ACI-2015-11-SOA-0157 |
| 18. | Ronda MCM, Dijkhorst-Oei L, Rutten GEHM. Reasons and barriers for using a patient portal: Survey among patients with diabetes mellitus. J Med Internet Res. 2014[cited];16(11):e263. https://doi.org/10.2196/jmir.3457 |
| 19. | Kruse CS, Karem P, Shifflett K, Vegi L, Ravi K, Brooks M. Evaluating barriers to adopting telemedicine worldwide: A systemic review. J Telemed Telecare. 2018;24(1):4–12. https://doi.org/10.1177/1357633X16674087 |
| 20. | CMS. Medicare Physician and Other Supplier National Provider Identifier (NPI) Aggregate Report, Calendar Year 2017. data.CMS.gov; 2019 [cited 2020 Mar 10]. Available from: https://data.cms.gov/Medicare-Physician-Supplier/Medicare-Physician-and-Other-Supplier-National-Pro/n5qc-ua94 |
| 21. | Digest of Education Statistics. National Center for Education Statistics (NCES) Home Page, a part of the U.S. Department of Education; 2017 [cited 2020 Mar 3]. Available from: https://nces.ed.gov/programs/digest/d17/tables/dt17_702.60.asp |
| 22. | Holm KE, Plaufcan MR, Ford DW, et al. The impact of age on outcomes in chronic obstructive pulmonary disease differs by relationship status. J Behav Med. 2014[cited];37(4):654–63. https://doi.org/10.1007/s10865-013-9516-7 |
Copyright Ownership: This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, adapt, enhance this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0.