Lauren M. Aiello, Sara Dadashzadeh, Jacob M. Lynn, William T. Starbird, Caleb J. Pawl, Silverberg Aryee, Henry R. Haley
Affiliations: Central Michigan University College of Medicine, Mount Pleasant, MI, USA
Corresponding Author: Lauren M. Aiello, Email: aiell1lm@cmich.edu
Keywords: Meta-Analysis, Psychiatric Disorder, Suicide, Telemedicine, Telepsychiatry
Objective: To review the published research for reported effectiveness of telemedicine in reducing suicide ideation and behavior in patients already diagnosed with a psychiatric disorder.
Design: A thorough literature search on the PubMed, Web of Science, PsycInfo, Cochrane Library, and TRIP (Turning Research Into Practice) Medical Database was conducted. Phrases such as “telemedicine,” “telehealth,” “remote consultation,” “mobile health,” “psychiatric disorders,” “suicide,” “suicide, attempted or ideation,” and “telepsychiatry” were employed in a variety of combinations. The primary inclusion criteria encompassed peer-reviewed articles published in the past 5 years. Secondary inclusion criteria comprised: (1) the diagnosis of any psychiatric disorder for all patients included in the study, (2) the absence or presence of use of telepsychiatry to offer consultation and communication, and (3) reported outcomes involving suicide rates or attempted suicide rates. The research publications passing inclusion criteria were assessed, and all their corresponding outcome measures were included in a meta-analysis.
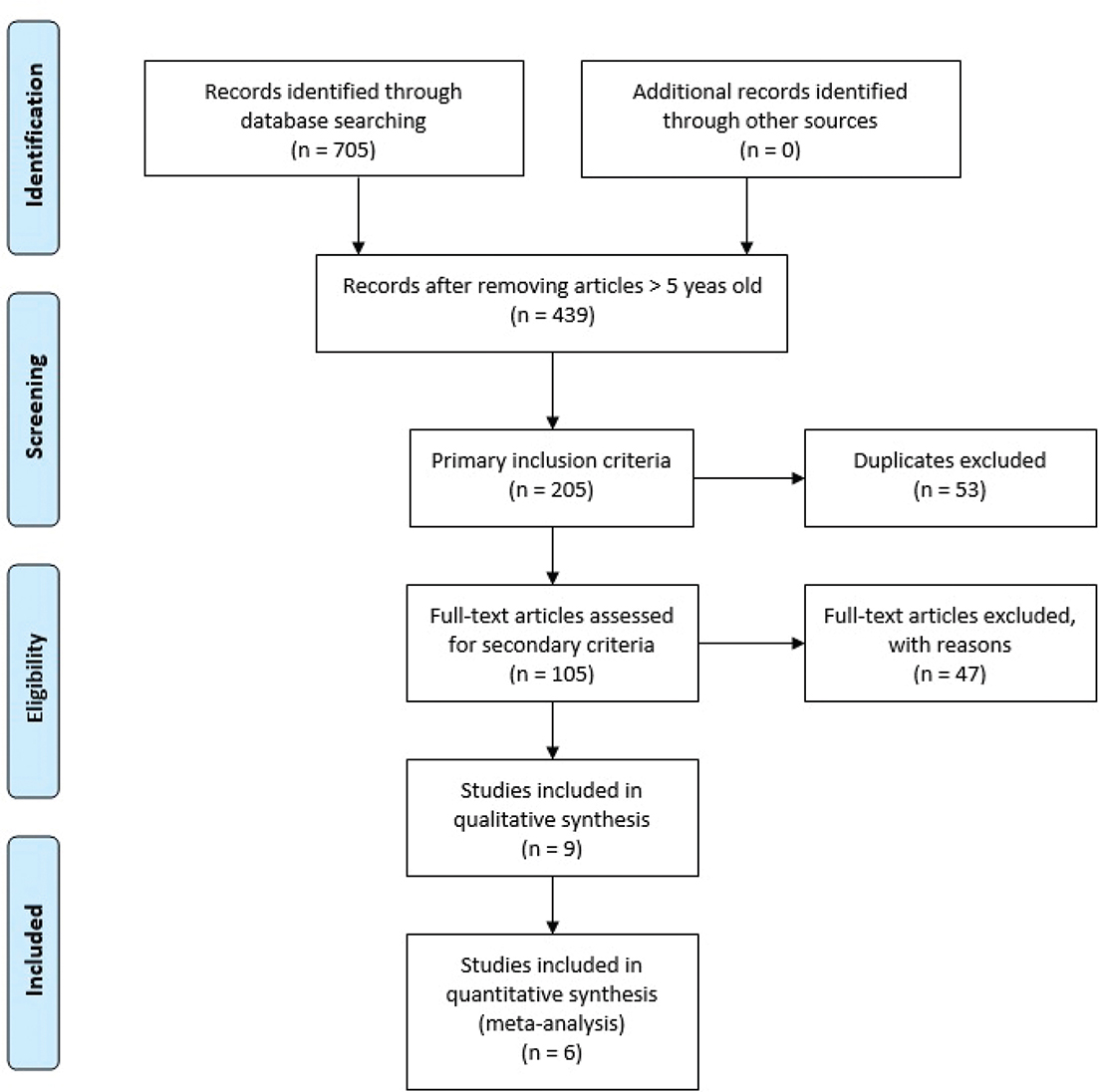
Results: A total of 705 studies were identified by applying the initial search strategy to the electronic databases described. Of these, 205 passed the primary inclusion criteria. After excluding duplicates and non-English articles, 105 articles were screened using the secondary inclusion criteria. Nine articles remained, including three systematic reviews that were excluded. Finally, a total of six independent, non-overlapping studies were included in this meta-analysis, encompassing data for 576 participants.
The 18 outcome measures in this meta-analysis included five “positive” measures: perceived ability to cope with suicidal ideation, optimism, gratitude, positive affect, and the Mini Mental State Exam. The “negative” measures included: suicidal ideation intensity, hopelessness, depression, suicidality, HAMD (Hamilton Depression Rating Scale) score, HAMD score without suicide item, medical admissions, number of days of medical hospitalizations, number of psychiatric hospitalizations, number of emergency room visits, suicide ideation questionnaire (SIQ) from baseline to posttreatment, and SIQ from baseline to follow-up. Overall, this review found support for the hypothesis that telemedicine can reduce suicide ideation and behavior. There was a moderate effect size for the 18 measures analyzed. Based on the four different forest plots presented in this analysis, all average effect sizes calculated showed that the intervention of telemedicine has a small-to-moderate effect on the measures studied, which translates loosely to a small-to-moderate effect on the patient’s suicide ideation and behavior.
Conclusions: Telemedicine appears to be a promising way to reduce suicidal ideation, although how this translates into reductions in self-harm and/or suicide attempts is unclear from this review alone.
Telemedicine can be defined as the use of telecommunication technologies to provide medical information and support health care when distance separates the participants.1 The definition of telemedicine includes not only the use of telephones to educate or provide for patients but also any type of remote electronic clinical consultation. Telemedicine includes any type of diverse technology to transfer medical information from one site to another. The idea of telemedicine has been controversial throughout the years. It can be viewed as a valuable tool for providing specialty care to underserved populations, a means of using medical resources to improve efficiency, and a way to provide health care to patients who may not be located near a hospital service area. On the other hand, it might be seen as a misallocation of increasingly scarce healthcare dollars. It is important for physicians to understand the principles of telemedicine as well as obstacles and limitations it might impose on the quality of treatment and the patient–physician relationship. Telemedicine can be used to transfer a wide range of medical information to both patients and other physicians at another location. For example, image transfer is an essential process for both radiology and pathology, and this information can be transferred quickly using telemedicine. Also, physical findings and specialized tests can be transferred, allowing for integrative examinations and even psychiatric interviews.2
The technique of telemedicine to transfer medical information to another site was first used in 1959 when Wittson and colleagues employed a two-way interactive television and used a microwave link for telepsychiatry consultation between the Nebraska Psychiatric Institute in Omaha and the state mental hospital, 112 miles away.3 Throughout the early years, until the 1990s, telemedicine was mainly being used for specialty consultations via videoconference technology. More recently, telemedicine has added a focus on noninteractive applications such as the use of store-and-forward technologies to save and transmit both images and documentation like a multimedia e-mail.4 At-home patient monitoring has also been incorporated into health care via telemedicine technologies by offering monitoring devices connected to computers that measure data including a patient’s blood pressure, heart rate, blood glucose level, pulse oximetry, and more. Even patients with limited education have been able to use these devices successfully to provide accurate results that can be transmitted back to their physician.5
Another interesting application of telemedicine technology is its use within ICUs. Parents of patients can check on their infants, who might be in the neonatal ICU, all the way from their home. They can obtain progress reports, live video visits, daily photographs, and email access with their child’s physician. This has been shown to greatly improve family satisfaction and lower cost for hospital-to-hospital transfers for the intervention group.6
Since October 1, 2001, Congress has acted to expand Medicare coverage of telemedicine to include more geographic regions as well as more physician services.7 Everything from consultations, office visits, individual psychotherapy, and pharmacologic management are covered with Medicare when they involve interactive audio and video. Although Congress has limited telemedicine coverage with Medicare and Medicaid to mainly rural areas, an increasing number of state Medicaid programs and private insurers have expanded coverage in recent years.4 Telemedicine is becoming such a mainstream and prevalent practice that some states such as California, Texas, and Louisiana have passed laws stating that insurers cannot have different reimbursement policies for those patients using telemedicine and for those using regular standard medical services.8 With the most common medical uses ranging from triage to consultation to diagnosis, telemedicine provides opportunity for healthcare growth by providing and expanding care to where it has previously been limited.
With regard to the topic of interest here, telemedicine can be used to improve access to mental healthcare and mental health specialists throughout the United States. Psychiatric disorders and mental illnesses are highly prevalent conditions found within the United States. According to the National Institute of Mental Health, one in five adults lives with some form of mental illness (ranging from mental illnesses that cause no to severe impairment). In 2017, that consisted of roughly 46.6 million adults aged 18 or older; of these adults, only 19.8 million received psychiatric care in the past year.9 Additionally, studies reveal that for every three to four children in the United States, at least one suffers from some sort of a mental disorder and about 1 in 10 may suffer from a serious emotional disturbance. However, very few will receive adequate mental health care required to treat and manage their condition.10 In fact, while nearly half of those who suffer from a chronic mental illness begin showing signs and symptoms at the age of 14 years, long delays exist between the onset and the seeking of treatment.11 Researchers estimate that there is a median delay of approximately 11 years after the initial onset of symptoms for any mental illness to first contact with a psychiatrist.
Severe mental illnesses generally have shorter delays but even then, many wait 5 years before seeking treatment. Such delays in treatment correlated with increased morbidity and mortality from either the development of various psychiatric and physical comorbidities or the adoption of coping and self-therapeutic methods that have a direct negative impact on health.12 Expansion of access to mental health services is crucial for avoiding the negative consequences associated with lack of treatment.
Suicide ideation, which includes general thoughts about suicide and even having a plan to act on these thoughts, is considered a mental process and a symptom of mental health illness.
The following statistics indicate that suicide is becoming a public health crisis. There are approximately 44,000 suicides every year in the United States. In 2017, 47,173 Americans died by suicide. Suicide is now the 10th leading cause of death in the United States overall and the third leading cause of death among 15–24 year olds. In addition, in 2015, suicide and self-injury cost in the United States was $69 billion.13
A recent comprehensive study conducted jointly by the Cohen Veterans Network and National Council for Behavioral Health on the access of mental health in America reported that while nearly 56% of those surveyed desire mental health services for themselves or for someone they care for, 74% do not believe mental health services are accessible. Barriers to treatment include high cost and insufficient insurance coverage, lack of awareness, social stigma, limited options, and long wait time. The survey revealed that 38% waited a week or more before receiving treatment, and 46% had to drive more than an hour round trip to receive treatment. Telemedicine can bridge this gap and allow more people who are considering seeking treatment to see providers more quickly and conveniently. In fact, 45% of Americans are open to try telehealth services for their current or future mental health need.14
Subsequently, follow-up with patients who are having suicide ideation or attempted suicide can yield positive outcomes. Thoughts of suicide linger among victims. Studies show that the risk of suicide is increased in the first week following discharge from psychiatric care, and frequent follow-ups are vital to prevent recurrence of suicidal behavior, ideally within 7 days after discharge.15 This is a gap that telemedicine can help bridge and help improve outcomes for patients living with mental health issues. As more and more people are open to seek mental health services and open to telemedicine as a way to access those services, it is important to understand how current use of telehealth impacts mental health treatment and, most importantly, how impactful it is in lowering the rates of suicide in the United States and changes needed to achieve that goal.
Suicide is the 10th leading cause of death in the United States and is also one of the top 10 causes of death among any age group.16 Ninety percent of those who die by suicide had previously demonstrated some sort of symptom of a mental health disorder.11
Alarmingly, the suicide rate in the United States is increasing steadily. The CDC (Centers for Disease Control) reports that the rate of death by suicide in the United States has increased by 33% from 1999 to 2017.17 While this increase is nationwide, there is an increasing disparity between the rate of suicide in rural communities compared with urban ones. Iglehart found that the death rate by suicide in rural counties was higher compared with the rates of suicide in metropolitan counties. The rate in rural counties was 17.32 per 100,000 compared with 14.86 in small-to-medium metropolitan counties and 11.92 in large metropolitan counties.18 One potential cause of this could be inadequate access to mental health resources such as crisis centers and physicians in rural areas compared with urban. However, the fact remains that improving access to mental health resources is applicable to both settings and is why we are exploring the potential use of telemedicine as a vital resource in providing care.
Suicide has historically been a taboo topic; however, public perceptions of mental health and suicide prevention are undergoing significant changes as evidenced by increasing numbers of organizations and advocates speaking out about the topic.19 Advocacy and social awareness have led to cultural changes such as using different terminology when discussing suicide. Examples of changes in terminology include avoiding the phrase “commit suicide” and instead say “died by suicide” or “ended his or her life” and stating that someone “attempted suicide” instead of referring to a successful or failed suicide attempt.19
The United States also has institutional changes to try to prevent suicide. Since 2006, 32 states have passed laws mandating kindergarten to 12th grade teacher training for signs among troubled children and the proper actions in the case of a student who may be contemplating suicide.19 Another powerful service available to our citizens is the American Foundation for Suicide Prevention’s Talk Saves Lives program. This organization and many others like it reaches people all over the United States, educating them about suicide as a health issue and its prevention. Their take home message is that just as we want patients to see their primary care physician (PCP) at the earliest signs of diabetes, for example, we want them to see their PCP at their earliest stage of mental deterioration or an increase in suicide risk.19
In theory, by speaking with physicians earlier, patients should be able to be directed to other mental health services, and suicide rates should be reduced. However, according to Rosenblatt et al., more than 50 million US citizens live in rural areas, and only 9% of the nation’s physicians’ practice in rural communities.20 Thus, even if we continue to create awareness and reduce the stigma surrounding suicide, nearly 20% of the population in the United States will not have proper access to healthcare providers to discuss their mental health issues.20 This is just one of many applications where telemedicine can be beneficial in reducing suicide rates in populations with reduced access to healthcare services.
Primary care clinics commonly attempt to treat underlying conditions as a suicide prevention method. They also refer patients to cognitive behavior therapy or dialectical behavior therapy. These methods show promise in decreasing the prevalence of attempted suicide.21 However, the 50 million Americans living in rural communities do not appear to benefit as much as those with better access to healthcare providers. Additionally, Rosenblatt et al. point out that “critical windows exist for suicide risk, including the week after a psychiatric admission, the week after a psychiatric discharge, discharge from an emergency department following presentation for suicidal ideation or attempt, and the first weeks after starting an antidepressant.”20 Ideally, patients consult their PCP during these high-risk periods. Unfortunately, this may not be possible due to inaccessibility. However, with the help of telemedicine physicians, their patients can be assessed for suicidal risk factors.
According to the Association of American Medical Colleges (AAMC), the United States physician shortage was estimated at 21,800 in 2017, and in response to an increasing population age, this deficit is expected to rise to as high as 122,000 in the year 2032.22 Of this deficit, the shortage of physicians is especially high for primary care and psychiatry providers.22 As this shortage in healthcare providers continues to rise, we are at risk for a healthcare crisis, involving a high healthcare demand without adequate supply to meet this demand. One potential solution is improving access to health care and telemedicine. As the practice of telemedicine continues to be adopted by healthcare institutions and used by patients nationwide, it is important to explore this relatively newer method of practicing medicine on patient outcomes.
A shortage of psychiatric health providers available is not the only problem the United States is facing. Increasing concerns about mental illness include rates of suicide. According to the CDC, age-adjusted suicide rates have increased by 33% from 1999 to 2017,17 with suicide ranking as the 10th leading cause of death within the United States for 2017.23 With this mind, exploring potential solutions for adequate access to psychiatric care for patients with suicide ideation is critical if we want to avoid a potential suicide crisis. Our project aims to provide a comprehensive review on how utilization of telepsychiatry services impacts patient healthcare outcomes with those with suicidal ideation and suicidal attempts.
A search of the literature with regard to suicide and telehealth in the past 10 years identified 14 previously conducted reviews. Of the reviews that most relevant to this topic, one focused solely on analyzing whether cognitive behavioral therapy (CBT) might be beneficial in reducing suicide ideation and behavior when delivered either in the traditional face-to-face method versus the newer telehealth mode. This study, conducted in 2017, reported CBT as useful in lowering suicide ideation and behaviors in the traditional face-to-face psychotherapy model. Due to lack of studies on CBT for suicide ideation and behavior in the telehealth setting, the researchers could not conduct a meta-analysis and where unable to determine whether CBT was effective in addressing suicide ideation and behavior when delivered via telemedicine. The authors expressed a need for a more in-depth look into the effects of telemedicine and its impact on suicide ideation and behavior.24
Another review investigated whether online suicide prevention programs can be effective. The studies evaluated were focused mainly on the effects of internet-based CBT, with some studies integrating regularly spaced assignments as well. The review determined that there is some evidence to suggest this format can be beneficial if the target is specifically suicidal content as opposed to depression, as suicidal ideation was reduced in many of the participants of the included studies. However, it was recommended that further research is required to form a more definitive stance on the effectiveness of this approach. It is worth noting that many of the studies analyzed excluded participants who were at high risk of attempting suicide or who were actively suicidal.25 Additional research found that CBT delivered over the internet by a therapist did decrease suicidal ideation, although not to the same extent as in-person therapy. However, it was found that various outcomes related to suicide, including thoughts, re-attempts, and mortality, were reduced by the addition of telephone management to usual care. The authors emphasize the lack of research on suicide prevention using technology in general.26
Another review evaluated whether mobile apps are effective for children and adolescents with mental health problems, including suicide. It was found that a lack of evaluation of the apps meant there was not enough evidence that they were effective for this age group. More research is needed to evaluate currently available and newly released mobile apps targeting mental health.27
Our literature review found that when it comes to reviews conducted on the topics of telemedicine and suicidal behaviors/ideations, research topics focus either on very specific treatment types (i.e., delivery of CBT or the use of other various technologies outside the traditional telehealth delivery system) or their impact on either suicide ideation or other mental health illnesses. Other reviews found in the literature search focused on topics irrelevant to determining whether telepsychiatry/telemedicine has an impact on suicide ideation and behavior. Therefore, it was determined that currently the field is lacking a review that focuses solely on the impact of telepsychiatry on suicidal ideation and suicide attempts. For this reason, this systematic review, which will look broadly into whether therapy delivered via telepsychiatry has aided in the reduction of suicidal ideation and suicide attempts, will add to the current literature by providing a broader view point on the topic.
Two types of studies were used in this meta-analysis: the first being a pre/post study and the second being randomized controlled trials. The time frame for the selection criteria as described in the methods is 5 years (i.e., June 2014–June 2019). The null hypothesis for this systematic review was that telemedicine neither impacts suicide attempts and/or suicide rates nor suicide ideation for those with a psychiatric disorder. The alternative hypothesis is that telemedicine will decrease both attempted and completed suicide rates as well as suicide ideation and/or behaviors for those diagnosed with psychiatric disorders when compared with those diagnosed with psychiatric disorders that used traditional in office therapy and/or consultation sessions.
A thorough literature search was conducted using PubMed, Web of Science, PsycInfo, Cochrane Library, and TRIP online database. Search phrases such as “telemedicine,” “telehealth,” “remote consultation,” “mobile health,” “psychiatric disorders,” “suicide,” “suicide, attempted or ideation,” and/or “telepsychiatry” were used in a variety of combinations. The PubMed database was searched using the following phrase: (suicide OR “attempted suicide” OR “suicide ideation” OR “suicidal ideation” OR “suicide, attempted or ideation” OR “suicide rates” OR “Suicidal Ideation”[MESH; i.e., (Medical Subject Headings)] OR “Suicide”[MESH] OR “Suicide/prevention and control”[MESH] OR “Suicide/psychology”[MESH] OR “Suicide/rehabilitation”[MESH] OR “Suicide/statistics and numerical data”[MESH] OR “Suicide/therapy”[MESH] OR “Suicide/trends”[MESH] OR “Suicide, Attempted”[MESH] OR “Suicide, Attempted/prevention and control”[MESH] OR “Suicide, Attempted/psychology”[MESH] OR “Suicide, Attempted/statistics and numerical data”[MESH] OR “Suicide, Attempted/therapy”[MESH] OR “Suicide, Attempted/trends”[MESH]) AND (telemedicine OR telehealth OR “online health” OR eHealth OR telepsychology OR telepsychiatry OR telemental OR “telemental health” OR teletherapy OR “Telemedicine”[MESH] OR “Telemedicine/methods”[MESH] OR “Telemedicine/statistics and numerical data”[MESH] OR “Telemedicine/trends”[MESH]). The other databases were searched using the following phrase: (suicide OR “attempted suicide” OR “suicide ideation” OR “suicidal ideation” OR “suicide, attempted or ideation” OR “suicide rates”) AND (telemedicine OR telehealth OR “online health” OR eHealth OR telepsychology OR telepsychiatry OR telemental OR “telemental health” OR teletherapy). The other databases included were Web of Science, PsychINFO, Cochrane, and TRIP.
Primary inclusion criteria were (1) studies must be published in the past 5 years, as the rate of change in technology is too great to consider older studies and (2) the studies must be peer reviewed. Secondary inclusion criteria include (1) the diagnosis of any psychiatric disorder for all patients included in the study, (2) the absence or presence of use of telepsychiatry to offer consultation and communication to those diagnosed with any psychiatric disorder, and (3) outcomes involving suicide rates or attempted suicide rates. Studies done outside of the United States and/or those not written in English were excluded. Articles that were already systematic reviews were also excluded.
The articles selected based on the primary literature search and the secondary criteria were evaluated for the classification of the type of community using telemedicine for psychiatric purposes and their associated outcomes. These included completed suicide rates and attempted suicide rates as well as many other measures. The articles including the aforementioned criteria and the desired outcomes needed for further analysis were included in this study.
In this systematic review, patients diagnosed with any psychiatric disorder of any age, gender, race, etc. either received telemedicine or no telemedicine. Those who did not receive telemedicine received traditional in-office therapy, consultation sessions, or no treatment. The outcomes of this review included suicide ideation and behavior and were determined based on an array of different measures from the articles analyzed. Six studies were included in this meta-analysis. The results reveal that telemedicine as an intervention had a small-to-moderate effect on the outcome measures studied, which can be interpreted as telemedicine having a small to moderate effect on suicide ideation and/or behaviors.
All members of our team participated in a primary search for articles based on the search phrases and primary criteria listed earlier. Then, two members of our team reviewed and performed an initial screening of all the articles selected, make sure that they fit the secondary criteria also listed above. A third member made the final decision for any articles that the two members disagreed on in the systematic review. Data extraction was then performed by two members for all the articles that meet the inclusion criteria. Data from this extraction were stored in Microsoft Excel. Another member analyzed and synthesized the data for the review. The statistical methods used to analyze and synthesize the data included mainly the Cohen’s d effect size calculations with the representation of these values on forest plots.
A total of 705 studies were identified by applying the initial search strategy to the electronic databases described in the “Methods” section to Web of Science (n = 84), PsychINFO (n = 176), PubMed (n = 162), Cochrane (n = 48), and TRIP (n = 235). After excluding articles that were older than 5 years, there was a total of 439 remaining records. Of these, 205 remained after considering the primary inclusion criteria explained in the “Methods” section. After excluding duplicates, the number was reduced to 152 articles. Of these, the non-English articles and/or those not written in the United States were excluded, leaving 105 articles that were screened considering the secondary inclusion criteria outlined in the “Methods” section. A total of nine articles remained with three of these being excluded due to being systematic reviews. Finally, a total of six independent, non-overlapping studies were included in the meta-analysis, encompassing data for 576 participants. Figure 1 is a flow diagram detailing the article selection process and results at each stage.
Figure 1—Flow diagram of included and excluded studies in the review.
All six of these studies were conducted in the United States. In terms of study design, three out of the six were pre/post studies28,29,30 and the remaining three studies were randomized controlled trials.31,32,33 Tables A1–A6 summarize pertinent characteristics of the six studies that were included in this review, including author, year, total participants (N), participant characteristics, study design, setting, intervention and control, and outcome measures. The average age of the participants was 48.21 (range 12–84). There was an average of 75.67 participants in the intervention group with a range of 20–296. There was an average of 78 participants in the control group with a range of 20–296.
The six studies were assessed, and all their corresponding measures were included in the meta-analysis. One of the studies did not report any mean or standard deviation data for any of their measures and thus their measures could not be included in this meta-analysis.28 Another study did not include the mean or standard deviation for their measure of at least one hospitalization and thus this measure was not included in the meta-analysis.33All other outcome measures reported in the Appendix were included in the meta-analysis for a total of 18 measures taken from five studies.
The 18 outcome measures include five “positive” measures: perceived ability to cope, optimism, gratitude, positive affect, and the Mini Mental State Exam. These five measures are classified as positive because a higher score corresponded to a reduced risk of suicide ideation and/or behavior. The remaining 13 outcome measures are classified as “negative” measures since the higher the score on the measure’s scale or rating system, the higher the likelihood for suicide ideation and/or behavior. They are suicidal ideation intensity, hopelessness,31,32 depression, suicidality, HAMD (Hamilton Rating Scale for Depression) score, HAMD score without suicide item, hopelessness, medical admissions, number of days of medical hospitalizations, number of psychiatric hospitalizations, number of ER visits, suicide ideation questionnaire (SIQ) from baseline to posttreatment, and SIQ from baseline to follow-up.
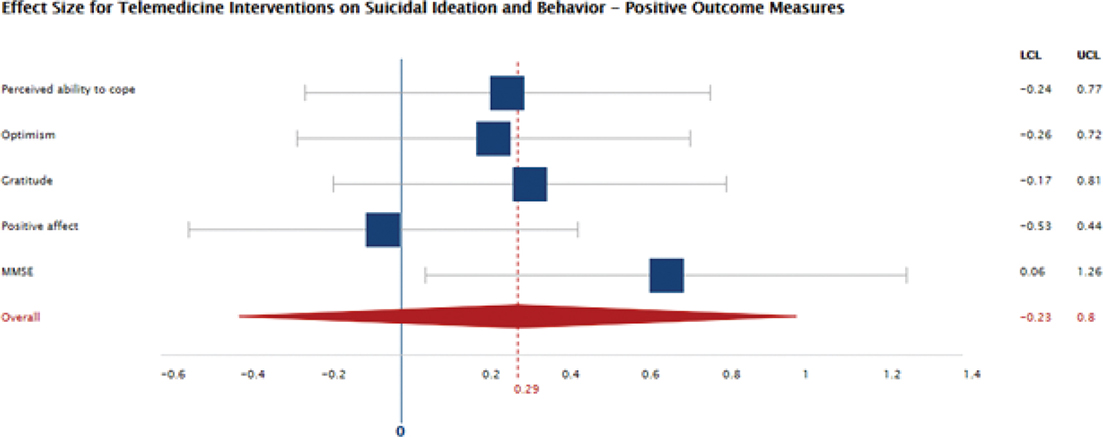
For each study, the effect size of telemedicine intervention was calculated for each of the study’s outcome measures. Effect size was calculated using Cohen’s d value (also known as the standardized mean difference). Figure 2 shows a forest plot of the mean effect size of telemedicine interventions on suicidal ideation and behavior for each positive outcome measure across the studies.
Figure 2—Effect size for telemedicine interventions on suicidal ideation and behavior—positive outcome measures.
As shown in Figure 2, the mean effect size for telemedicine interventions on suicidal ideation and behavior based on the five positive measures spreading across three of the studies with a total of 141 participants was 0.29, 95% CI, -0.23 to 0.80, which indicates a small-to-moderate effect. All effect sizes greater than zero in Figure 2 for the positive measures should be interpreted as the intervention of telemedicine improved the positive measures, decreasing the likelihood of suicide ideation and/or behavior. It is important to note that the confidence interval for the mean effect size as seen in Figure 2 does include a portion of negative numbers, meaning that telemedicine could have negatively impacted these positive measures as an intervention. Also, there is one measure (positive affect).31 This would indicate that the employed telephone-based positive psychology intervention negatively impacted the propensity to experience positive emotions and interact with others in a positive way.
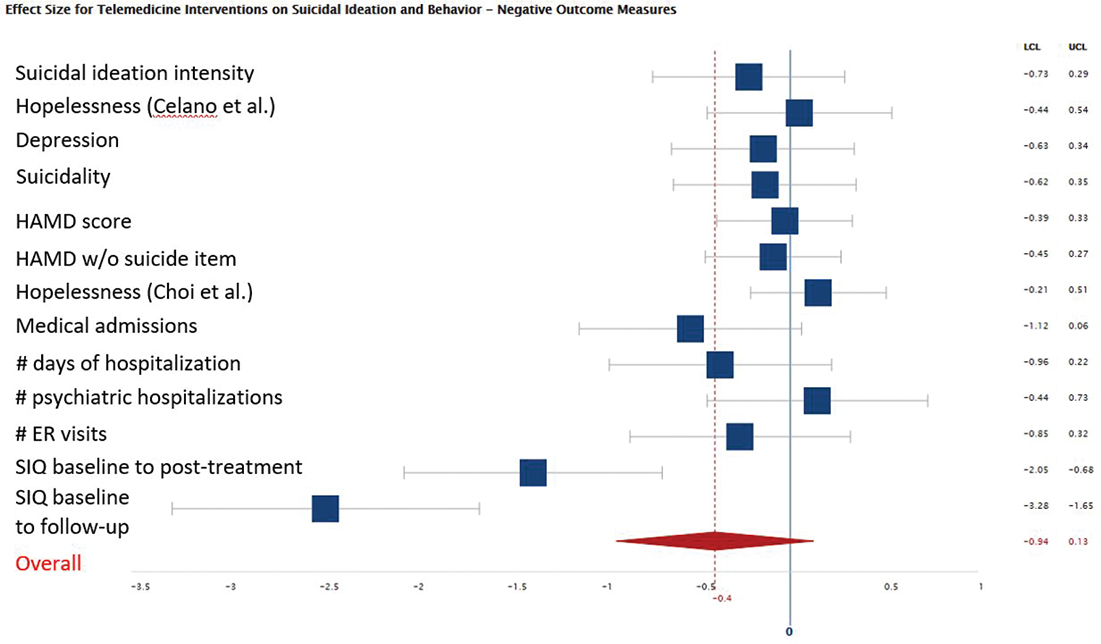
Figure 3 presents the forest plot for the 13 negative measures analyzed in this meta-analysis involving five of the studies and 280 participants. The average effect size for the negative measures was -0.40 with a 95% CI of -0.94 to 0.13, which can be interpreted as a moderate effect. All effect sizes less than zero, or negative, for this figure should be interpreted as the intervention of telemedicine lowered the scores and/or ratings for these measures, meaning that there was a decreased likelihood of suicide ideation and/or behavior. Similarly, to the first forest plot’s confidence interval, the confidence interval for the average effect size of the negative measures contains positive numbers, meaning that the telemedicine could have increased these negative measures. In other words, the intervention of telemedicine could have negatively impacted a person’s suicide ideation and/or behavior. It should also be noted that three measures in this plot had positive effect sizes, also meaning that telemedicine as an intervention negatively impacted and increased the risk for a person’s suicide ideations and/or behaviors. These measures were hopelessness,31,32 and number of psychiatric hospitalizations.33
Figure 3—Effect size for telemedicine interventions on suicidal ideation and behavior—negative outcome measures.
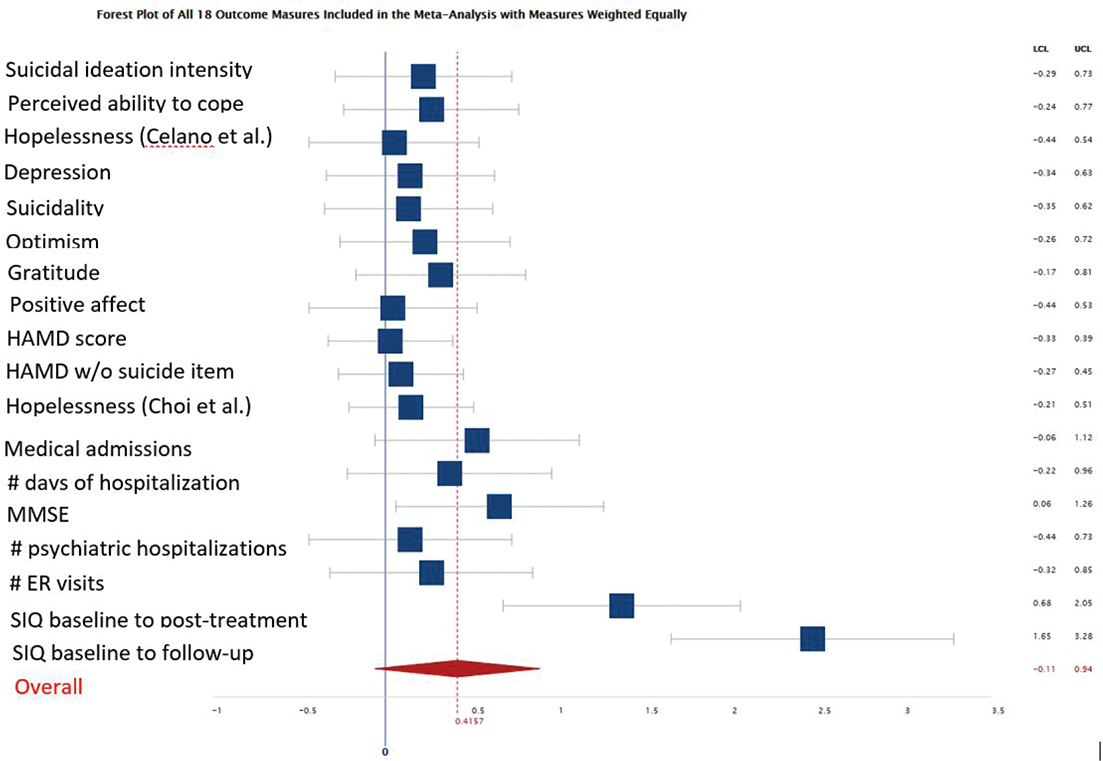
To combine positive and negative outcome measures analyzed, the absolute value was taken for all the effect sizes. Therefore, a positive effect size would now indicate that the intervention of telemedicine was beneficial to the patient, in that it either increased the positive measures and/or decreased the negative measures when compared with the control group. For example, with the intervention of telemedicine, the patients had a lower score on the SIQ than they did prior to treatment and the patients had a higher sense of gratitude and optimism. Thus, in this forest plot, all the measures are weighted equally to get a final average effect size. Figure 4 presents the resulting forest plot with all 18 measures weighted equally. The overall average effect size for all 18 measures being 0.416, which can be interpreted as a moderate effect with a 95% CI of −0.11 to 0.94. This confidence interval does contain a small interval of negative numbers, which can be interpreted as there being a small chance that telemedicine was an intervention that was negatively affected and thus increased the risk for suicide ideations and/or behaviors.
Figure 4—Forest plot of all 18 outcome measures included in the meta-analysis with measures weighted equally.
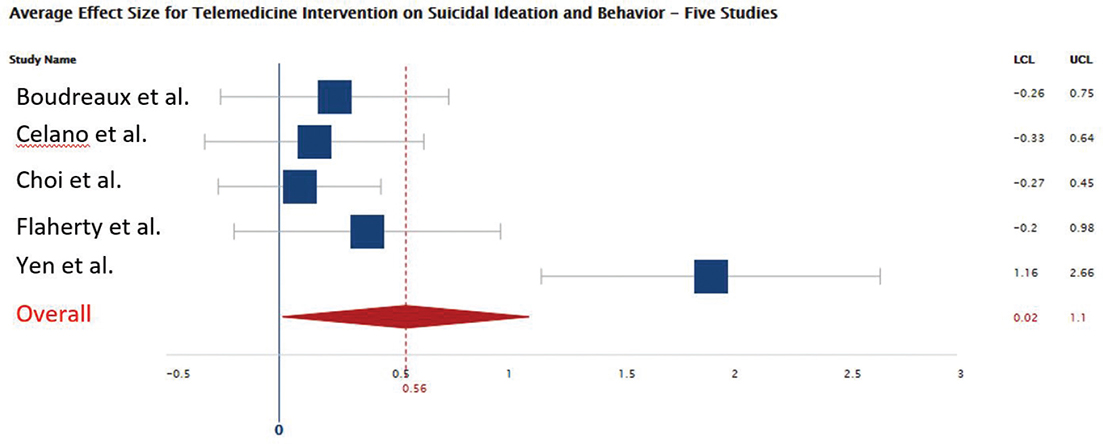
In another effort to compare each study equally and not put too much weight on one study due to their large amount of measures, another forest plot was created to show the effect size for each study by averaging all their measure’s effect sizes. The forest plot in Figure 5 shows each study’s average effect size for all outcome measures considered by the study allowing for the studies to be weighted equally. For example, the three effect sizes and their limits for each measure in Choi (2016) were averaged to create one effect size for the study done by Choi (2016). There is not an effect size for Bauer (2016) because as mentioned before for each measure conducted in this study, there were no reported means and/or standard deviations.28 Also included in this forest plot, (Figure 5) there is another average effect size with each article being weighted equally. This has an effect size of 0.56 (95% CI, 0.02–1.10), which can be interpreted as a moderate effect. This is the only forest plot whose average effect size has a confidence interval that only includes positive numbers. This means that 95% of the time the average effect size will be positive, meaning that the intervention of telemedicine positively affected the person’s suicide ideation and/or behavior based on all 18 measures studied.
Figure 5—Forest plot of average effect size for telemedicine intervention on suicidal ideation and behavior in five studies.
This systematic review and meta-analysis evaluated the effectiveness of telemedicine and digital interventions for the management and/or treatment of suicidal ideations or behaviors. A total of six studies were included in this review with a total of 576 participants.
Overall, this review confirmed the hypothesis that telemedicine can reduce suicide ideation, and suicidal behavior is somewhat supported. There was a moderate effect size for the 18 measures analyzed for the independent studies although there was significant heterogeneity between the included studies and their respective outcome measures. All but one of the forest plots and average effect sizes calculated have a confidence interval that only included a range of numbers that could be interpreted as telemedicine, helping to reduce suicide ideations and/or behaviors. The effects for the telemedicine intervention tended to be stronger in the pre/post studies when compared with the randomized controlled studies. A few of the studies noted that the adherence to the digital intervention was poor. For example, in one study only 296 participants out of the initial 379 consults (78.1%) completed the digital intervention of clinical video teleconferencing.28 This could suggest that the use of digital interventions may not be sufficient enough and/or engaging enough for long-term therapy.
There was also a moderate effect size for the five articles weighted equally, as seen in Figure 5, being interpreted as the intervention of telemedicine helping decrease suicide ideation and other measures that are similar. The lower limit of the 95% confidence interval is 0.02, which is a positive number meaning that the telemedicine intervention helped to reduce suicide ideation and/or behavior.
As discussed previously, the literature involving the effects of telemedicine on suicidal ideation and behavior is lacking. Previous systematic reviews tended to focus on narrow avenues of treatment, such as CBT.24–26 Others investigated the effects of intriguing new mobile applications that hypothetically could provide treatment regardless of patient location. However, the authors found that the data supporting their implementation are insufficient.27 Important to note is that previous systematic reviews were limited on this topic to either suicidal ideation or foci related to suicide, such as depression scores. Many previous studies outright exclude participants deemed to be at high risk of suicide. As far as we know based on literature review, the current study is the first systematic review to include analysis of the effects telemedicine has on suicidal behavior in addition to the other factors just mentioned. This is an important step in quantifying the benefits telemedicine may offer in reducing suicide prevalence, especially considering the ability it can offer physicians to reach patients who are otherwise too distant to receive care.
A strength of this analysis is that it presents a broader review of the literature on the effects of telemedicine (specifically administered by a healthcare professional) on suicide ideation/attempts. Previous studies tended to be either more specific to individual treatment modalities, such as CBT via video-chat, whereas the current analysis attempted to include any modality that utilized a healthcare provider outside of the typical in-office visit. In addition, previous studies tended to focus on mental health illnesses as a whole rather than suicide ideation/attempts. The current analysis, as far as we know, is the first to examine the effects of telemedicine on suicide risk behaviors, in addition to the focus on suicidal ideation. Additionally, to ensure a comprehensive review on the topic, five databases were consulted in this study. This study also avoided bias by utilizing two different reviewers of all articles gathered with the aid of an independent tie-breaker when determining relevant studies for the review. Telemedicine is quite new to the medical field due to the advancements made in technology in the past 5 years. Thus, this meta-analysis provides a baseline and an understanding of the capabilities of telemedicine for patients with psychiatric disorders. This analysis is a stepping stone for many future studies related to the benefits of telemedicine.
A limitation of this analysis is the small number of studies included in the meta-analysis. Future analyses could improve upon this by expanding the inclusion criteria to include variables not limited to only suicide ideation and behavior, but perhaps variables shown in other studies to be related to suicide ideation and behavior. Another limitation to this analysis is the lack of clarity regarding the extent to which participants who have suicide ideation/behaviors are comparable to those who have completed suicide.
The wide heterogeneity of both the clinical settings and the different methodology and measures used in each study is another limitation that made it difficult to complete the meta-analysis without weighting the results. For example, it was difficult to compare the positive versus negative measures in a reasonable way. There were many different outcome measures used in this study, which add to the heterogeneity. All the articles used in this meta-analysis had a different way to measure suicide ideation. Some used surveys to collect information and others used data regarding medication use or hospital stays. The outcome measures were separated into positive and negative measures as described earlier to make meaning out of our analysis despite the heterogeneity. For future studies, having the same survey or outcome measure for suicide ideation would be ideal in addressing some of the clinical heterogeneity seen in this meta-analysis.
There is also a clinical heterogeneity seen regarding the broad age of participants and wide variety of psychiatric disorders in the studies included. It is unclear whether the wide range of ages in the studies could have contributed to the results of the current study, as there are conflicting studies regarding telemedicine and age. One study showed that patient’s age is one of the most common barriers listed for the adoption of telemedicine,34 while other studies found that patient age does not predict whether or not a patient will find telemedicine as good or better than traditional visit.35 It has been demonstrated that suicide rates are higher in the middle-aged and elderly population compared with the younger population.36 Therefore, it is possible but not clear whether age would have contributed to the outcomes measured. Regarding the type of psychiatric disorders, it is reported that between 12% and 19% of patients with depression will attempt suicide, compared with 5% and 14% in patients with schizophrenia.36 Therefore, it is possible the varying psychiatric diagnoses present in the current study could have contributed to the heterogeneity.
Clinical settings may have an effect on the outcome. It was found that suicide rates of patients with depression who are treated in the inpatient setting are about double those in the outpatient setting,37 so it is possible that the combination of inpatient and outpatient settings in the current study contributed to the heterogeneity. Similarly, different treatment settings and study locations, for example the urban tertiary care compared to a multicenter study with rural community clinics, would each pose unique challenges and patient populations, as factors such as rural settings have demonstrated to affect the effective telemedicine services.34 Additionally, the variety of treatment modalities could conceivably drive heterogeneity in the data, as it would be reasonable to expect different challenges, strengths, and outcomes among teleconferencing, telephone calls, and web-based delivery of mental health treatment.
Methodological heterogeneity is also present in this meta-analysis, as two different types of studies were used: randomized control trials and pre/post studies, the latter of which would not be able to rule out the possibility of extraneous factors impacting the findings. Due to the limited number of studies found on telemedicine being used to treat psychiatric disorders and its effect on suicide ideation, all six studies that passed the primary and secondary inclusion criteria were included regardless of the type of study. This adds moderate methodological heterogeneity although it is not believed to be substantial. According to the Cochrane manual, methodological heterogeneity contends that differences in methodological factors like adequate randomization, allocation concealment, and the use of blinding among studies will lead to differences in observed treatment effects, but these differences do not necessarily indicate that the true intervention effect varies.38 As more studies regarding telepsychiatry are published in the future, further research using the same type of methodology would be ideal for completing a meta-analysis that can avoid methodological heterogeneity. Lastly, it is difficult to determine the adequacy of the outcome measures used in assessing the efficacy of telemedicine (based on optimism, depression, hospital stays, etc.) are sensitive enough to change a person’s suicidal thoughts and/or behaviors and to what extent.
Telemedicine, delivered in a wide range of ways, appears to be a promising way to reduce suicidal ideation and has long been recognized as integral to the solution to rural health disparities, although how this translates into reductionsin self-harm and/or suicide attempts is unclear from this review alone. Based on the four different forest plots presented in this analysis, all average effect sizes calculated showed that the intervention of telemedicine has a small-to-moderate effect on the measures studied, which translates loosely to a small-to-moderate effect on the person’s suicide ideation and/or behaviors.
Although all average effect sizes seemed to show that telemedicine positively helped the patient when compared with traditional psychotherapy or in-office visits, only one had a 95% confidence interval that showed this to be true since its interval only included a range of numbers that showed telemedicine decreased a risk for suicide ideation/behaviors.
This meta-analysis provides a baseline understanding of the capabilities of telemedicine for patients with psychiatric disorders. It is the hope that this analysis shall become a steppingstone for any future studies that may wish to look at the benefits of telemedicine either related to suicide ideation/behavior or other benefits as well. The growing political exigency for long-term reform of public health funding should anoint telemedicine as the linchpin in the solution to rural health disparities—addressing poor access to mental health care and the overlapping public health problems of drug abuse and suicide.
Acknowledgments: The authors wish to acknowledge the following individuals whose efforts contributed to the success of the project: Dr Ariel Cascio, Dr Beth Bailey, Dr Neli Ragina, and Rebecca Renirie.
Funding Statement: The authors received no financial support for the research, authorship, and/or publication of this article. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Conflicts of Interest: The authors declare no potential conflicts of interest.
Contributors: All authors are 3rd year medical students at College of Medicine, Central Michigan University. All authors contributed to developing the research question and conducting the initial literature review, narrowing down articles based on the primary inclusion criteria. LA retrieved articles from PubMed, JL retrieved articles from Web of Science, WS retrieved articles from PsychInfo, SA retrieved articles from Cochrane Library, and HH retrieved articles from TRIP medical database. SD and JL independently reviewed these articles and narrowed them down based on the secondary inclusion criteria. CP was the tiebreaker for any discrepancies between the final list of articles that SD and JL came up with. WS and SA extracted the data from the six articles used in this meta-analysis. LA managed the extraction database and conducted the statistical analysis. HH and LA supervised the writing of the manuscript. All authors have approved this manuscript.
| 1. | Institute of Medicine. Telemedicine: A guide to assessing telecommunications for healthcare [Internet]. In: Field MJ, editor. Washington, DC: National Academies Press; 1996. Available from: https://pubmed.ncbi.nlm.nih.gov/20845554/ |
| 2. | Perednia DA, Allen A. Telemedicine technology and clinical applications. JAMA. 1995;273(6):483–8. http://dx.doi.org/10.1001/jama.1995.03520300057037 |
| 3. | Grigsby J, Kaehny MM. Analysis of expansion of access to care through use of telemedicine and mobile health services. Report 1: Literature review and analytic framework. Denver, CO: Center for Health Policy Research; 1993. |
| 4. | Field MJ, Grigsby J. Telemedicine and remote patient monitoring. JAMA. 2002;288(4):423–5. http://dx.doi.org/10.1001/jama.288.4.423 |
| 5. | Finkelstein J, Cabrera MR, Hripcsak G. Internet-based home asthma telemonitoring. Chest. 2000;117(1):148–55. http://dx.doi.org/10.1378/chest.117.1.148 |
| 6. | Gray JE, Safran C, Davis RB, et al. Baby CareLink: Using the Internet and telemedicine to improve care for high-risk infants. Pediatrics. 2000;106(6):1318–24. http://dx.doi.org/10.1542/peds.106.6.1318 |
| 7. | Department of Health and Human Services, Centers for Medicare and Medicaid Services. Program memorandum intermediaries/carriers [Internet]. 2002. Available from: https://www.cms.gov/Regulations-and-Guidance/Guidance/Transmittals/Downloads/AB02052.pdf |
| 8. | Office for the Advancement of Telehealth. 2001 report to congress on telemedicine: Payment issues [Internet]. Rockville, MD: US Dept of Health and Human Services; 2001 [cited 2019 May]. Available from: http://telehealth.hrsa.gov/pubs/report2001/pay.htm#tab1 |
| 9. | The National Institute of Mental Health. Mental illness [Internet]. The National Institute of Mental Health; 2019 [cited 2019 May 6]. Available from: https://www.nimh.nih.gov/health/statistics/mental-illness.shtml |
| 10. | Merikangas KR, He J-P, Burstein M, et al. Lifetime prevalence of mental disorders in U.S. adolescents: Results from the National Comorbidity Survey Replication-Adolescent Supplement (NCS-A). J Am Acad Child Adolesc Psychiatry. 2010;49(10):980–9. http://dx.doi.org/10.1016/j.jaac.2010.05.017 |
| 11. | National Alliance on Mental Illness. Mental health by the numbers [Internet]. Nami.org; 2019 [cited 2019 May 11]. Available from: https://www.nami.org/mhstats |
| 12. | McLaughlin CG. Delays in treatment for mental disorders and health insurance coverage. Health Serv Res. 2004;39(2):221–4. https://dx.doi.org/10.1111/j.1475-6773.2004.00224.x |
| 13. | American Foundation for Suicide Prevention. Suicide statistics [Internet]. Afsp.org.; 2019 [cited 2019 Apr 16]. Available from: https://afsp.org/suicide-statistics/ |
| 14. | Cohen Veterans Network & National Council for Behavioral Health. New study reveals lack of access as root cause for mental health crisis in America [Press Release]. Cohenveteransnetwork.org.; 2018 [cited 2019 May 13]. Available from: https://www.cohenveteransnetwork.org/wp-content/uploads/2018/10/Press-Release-Americas-Mental-Health-2018-FINAL.pdf |
| 15. | Jennifer S, Larry C. Suicidal ideation and behavior in adults [Internet]. Uptodate.com.; 2019 [cited 2020 Apr]. Available from: https://www.uptodate.com/contents/suicidal-ideation-and-behavior-in-adults |
| 16. | Mohatt NV, Billera M, Demers N, Monteith LL, Bahraini NH. A menu of options: Resources for preventing veteran suicide in rural communities. Psychol Serv. 2018;15(3):262–9. http://dx.doi.org/10.1037/ser0000203 |
| 17. | Hedegaard H, Curtin SC, Warner M. Suicide mortality in the United States, 1999-2017 [Internet]. 2018, p. 1–8. Available from: https://www.cdc.gov/nchs/data/databriefs/db330-h.pdf |
| 18. | Iglehart JK. The challenging quest to improve rural health care. N Engl J Med. 2018;378(5):473–9. http://dx.doi.org/10.1056/NEJMhpr1707176 |
| 19. | National Academies of Sciences, Engineering, and Medicine, Division of Behavioral and Social Sciences and Education, Board on Children, Youth, and Families, Health and Medicine Division, Board on Healthcare Services. Improving care to prevent suicide among people with serious mental illness: Proceedings of a workshop [Internet]. In: S Olson, editor. Washington, DC: National Academies Press; 1969. Available from: https://www.ncbi.nlm.nih.gov/books/NBK540131/ |
| 20. | Rosenblatt RA, Hart LG. Physicians and rural America. West J Med. 2000;173(5):348–51. http://dx.doi.org/10.1136/ewjm.173.5.348 |
| 21. | Gregory C. Suicide and suicide prevention [Internet]. Psycom.net.; 2019 [cited 2019 May]. Available from: https://www.psycom.net/depression.central.suicide.html |
| 22. | Dall T, West T, Chakrabarti R, Reynolds R, Iacobucci W. Update the complexities of physician supply and demand: Projections from 2016 to 2030 Final Report Association of American Medical Colleges [Internet]. Association of American Medical Colleges; 2018. Available from: https://www.researchgate.net/publication/331555846_2018_Update_The_Complexities_of_Physician_Supply_and_Demand_Projections_from_2016_to_2030_Final_Report_Association_of_American_Medical_Colleges |
| 23. | Murphy SL, Xu J, Kochanek KD, Arias E. Mortality in the United States, 2017. NCHS Data Brief [Internet]. 2018;328:1–8. Available from: http://www.cdc.gov/nchs/data/databriefs/db328-h.pdf |
| 24. | Leavey K, Hawkins R. Is cognitive behavioural therapy effective in reducing suicidal ideation and behaviour when delivered face-to-face or via e-health? A systematic review and meta-analysis. Cogn Behav Ther [Internet]. 2017;46(5):353–74. Available from: http://www.tandfonline.com/doi/full/10.1080/16506073.2017.1332095 |
| 25. | Christensen H, Batterham PJ, O’Dea B. E-health interventions for suicide prevention. Int J Environ Res Public Health. 2014;11(8):8193–212. http://dx.doi.org/10.3390/ijerph110808193 |
| 26. | Kreuze E, Jenkins C, Gregoski M, et al. Technology-enhanced suicide prevention interventions: A systematic review. J Telemed Telecare. 2017;23(6):605–17. http://dx.doi.org/10.1177/1357633X16657928 |
| 27. | Grist R, Porter J, Stallard P. Mental health mobile apps for preadolescents and adolescents: A systematic review. J Med Internet Res. 2017;19(5):e176. http://dx.doi.org/10.2196/jmir.7332 |
| 28. | Bauer MS, Krawczyk L, Miller CJ, et al. Team-based telecare for bipolar disorder. Telemed J E Health. 2016;22(10):855–64. http://dx.doi.org/10.1089/tmj.2015.0255 |
| 29. | Boudreaux ED, Brown GK, Stanley B, Sadasivam RS, Camargo CA, Miller IW. Computer administered safety planning for individuals at risk for suicide: Development and usability testing. J Med Internet Res. 2017;19(5):e149. http://dx.doi.org/10.2196/jmir.6816 |
| 30. | Yen S, Ranney ML, Tezanos KM, et al. Skills to enhance positivity in suicidal adolescents: Results from an open development trial. Behav Modif. 2019;43(2):202–21. http://dx.doi.org/10.1177/0145445517748559 |
| 31. | Celano CM, Beale EE, Mastromauro CA, et al. Psychological interventions to reduce suicidality in high-risk patients with major depression: A randomized controlled trial. Psychol Med. 2017;47(5):810–21. http://dx.doi.org/10.1017/S0033291716002798 |
| 32. | Choi NG, Marti CN, Conwell Y. Effect of problem-solving therapy on depressed low-income homebound older adults’ death/suicidal ideation and hopelessness. Suicide Life Threat Behav. 2016;46(3):323–36. http://dx.doi.org/10.1111/sltb.12195 |
| 33. | Flaherty LR, Daniels K, Luther J, Haas GL, Kasckow J. Reduction of medical hospitalizations in veterans with schizophrenia using home telehealth. Psychiatry Res. 2017;255:153–5. http://dx.doi.org/10.1016/j.psychres.2017.05.024 |
| 34. | Scott Kruse C, Karem P, Shifflett K, Vegi L, Ravi K, Brooks M. Evaluating barriers to adopting telemedicine worldwide: A systematic review. J Telemed Telecare. 2018;24(1):4–12. http://dx.doi.org/10.1177/1357633X16674087 |
| 35. | Polinski JM, Barker T, Gagliano N, Sussman A, Brennan TA, Shrank WH. Patients’ satisfaction with and preference for telehealth visits. J Gen Intern Med. 2016;31(3):269–75. http://dx.doi.org/10.1007/s11606-015-3489-x |
| 36. | Bachmann S. Epidemiology of suicide and the psychiatric perspective. Int J Environ Res Public Health. 2018;15(7):1425. http://dx.doi.org/10.3390/ijerph15071425 |
| 37. | Bertolote JM, Fleischmann A, De Leo D, Wasserman D. Psychiatric diagnoses and suicide: Revisiting the evidence. Crisis. 2004;25(4):147–55. http://dx.doi.org/10.1027/0227-5910.25.4.147 |
| 38. | West SL, Gartlehner G, Mansfield AJ, et al. Comparative effectiveness review methods: Clinical heterogeneity [Internet]. Rockville, MD: Agency for Healthcare Research and Quality; 2010. Available from: https://pubmed.ncbi.nlm.nih.gov/21433337/ |
Copyright Ownership: This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, adapt, enhance this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0.
Table A1. Study characteristics of “team-based telecare for bipolar disorder”28
| Bauer et al.28 | |
|---|---|
| Study design | Pre–post study |
| Setting | 8 VA regional networks and 11 states including small, rural community-based clinics |
| Participants | Veterans enrolled in VA outpatient care with known or suspected bipolar spectrum disorders, including cyclothymia and schizoaffective disorder, without other exclusion criteria |
| Total participants | N = 400 |
| Intervention and control | Intervention: clinical video teleconferencing (CVT) Control: before CVT |
| Outcome measures |
|
Table A2. Study characteristics of “computer-administered safety planning for individuals at risk for suicide”29
| Boudreaux et al.29 | |
|---|---|
| Study design | Pre–post study |
| Setting | Urban, tertiary care hospital in central Massachusetts |
| Participants | Presenting adult patients being evaluated for an acute psychiatric emergency in either the ED or the inpatient psychiatric unit |
| Total participants | N = 30 |
| Intervention and control | Intervention: a self-administered web-based safety planning application Control: before application |
| Outcome measures |
|
Table A3. Study characteristics of “psychological interventions to reduce suicidality”31
| Celano et al.31 | |
|---|---|
| Study design | Randomized controlled trial |
| Setting | Not specified |
| Participants | Patients with a primary diagnosis of major depressive disorder with a current major depressive episode, and expressed suicidal ideation on admission or following a suicide attempt |
| Total participants | N = 65 |
| Intervention and control | Intervention: telephone-based positive psychology intervention Control: cognition-focused control intervention |
| Outcome measures |
|
Table A4. Study characteristics of “effect of problem-solving therapy on … death/suicidal ideation and hopelessness”32
| Choi et al.32 | |
|---|---|
| Study design | Randomized controlled trial |
| Setting | Not specified |
| Participants | English speaking, non-Hispanic white, black, or Hispanic homebound adults aged 50+ with moderately severe-to-severe depressive symptoms (a score of 15+ on the 24-item HAMD for depression) |
| Total participants | N = 158 |
| Intervention and control |
|
| Outcome measures |
|
Table A5. Study characteristics of “reduction of medical hospitalizations in veterans with schizophrenia using home telehealth”33
| Flaherty et al.33 | |
|---|---|
| Study design | Randomized controlled trial |
| Setting | Not specified |
| Participants | Veterans with schizophrenia or schizoaffective disorder with suicidal behavior admitted for psychiatric care |
| Total participants | N = 45 |
| Intervention and control | Intervention: intensive care monitoring + telehealth monitoring Control: intensive care monitoring |
| Outcome measures |
|
Table A6. Study characteristics of “skills to enhance positivity in suicidal adolescents”30
| Yen et al.30 | |
|---|---|
| Study design | Pre–post study |
| Setting | Not specified |
| Participants | Participants recruited from an adolescent psychiatric inpatient unit, who were admitted due to concerns of suicide risk |
| Total participants | N = 20 |
| Intervention and control | Intervention: skills to enhance positivity (STEP), a two-part positive affect program with an in-person phase and a remote delivery phase Control: before STEP |
| Outcome measures |
|