Rachel M. Segal, BS1, Jared Matson, MD2, Omid Moshtaghi, MD3, Elina Vaidya3, Elina Kari, MD3, Rick Friedman, MD3, Sonia Ramamoorthy, MD2, Jeffrey P. Harris, MD, PhD3
Affiliations: 1UC San Diego School of Medicine, San Diego, CA, USA; 2Division of Colon and Rectal Surgery, UC San Diego Department of Surgery, San Diego, CA, USA; 3Division of Otolaryngology, Head and Neck Surgery, UC San Diego Department of Surgery, San Diego, CA, USA
Corresponding Author: Jeffrey P. Harris, Email: jpharris@health.ucsd.edu
Keywords: Colorectal Surgery, COVID-19, Otolaryngology, Neurotology, Surgery, Telehealth, Telemedicine
Section: Original clinical research
Background: During the COVID-19 pandemic, measures were taken to decrease viral spread by transitioning health care appointments to virtual mediums. This study evaluates the use of telemedicine within the Divisions of Colon and Rectal Surgery and Otolaryngology-Neurotology at a single academic institution during the COVID-19 pandemic.
Study Design: An online survey modeled after the TeleENT Satisfaction Questionnaire and the Medical Communication Competence Scale (MCCS) was administered to gauge patient’s experience with Electronic Medical Record-based telemedicine visits.
Results: Participants noticed several advantages of telemedicine visits over traditional in-office visits: shorter visits, saving money, and avoiding potential exposure during the pandemic. A total of 36% at least somewhat agreed that the quality of care was hindered by the lack of a physical examination;61.7% participants at least somewhat agreed that they prefer a face-to-face visit rather than telemedicine consultation. Most patients were satisfied with the care they received via telemedicine (Likert 6.19/7) and 95.8% would use telemedicine again. Participants self-reported an average saving of $108.70 when using telemedicine. When comparing the telemedicine cohort with the in-office control, the telemedicine patients noticed an improved ability to communicate with their physician in five out of eight domains of the MCCS.
Conclusion: Surgical preoperative consultation, postoperative follow-up, and routine visits were conducted via telemedicine during the COVID-19 pandemic, representing a new direction for surgical appointments and consultations. This study shows that telehealth can provide satisfactory care and increases access to surgical care for patients when external factors prevent the traditional physician–patient interaction. With better-perceived communication via telemedicine appointments, patients may subjectively feel that they can express their symptoms and gather information from the doctor regarding their diagnosis more efficiently.
Telehealth is the distribution of health-related services and information via electronic information and telecommunication technologies. Telemedicine has seen increased interest in recent years, particularly with the centralization of specialized care in high-volume centers and the increased prevalence of smart devices.1,2 Studies show that it allows for improved access to specialty care for patients in rural areas, decreased travel time, cost-savings, reduced wait times, higher patient satisfaction, and improved clinical efficiency.3–10
Recently, telemedicine has been used in a wide range of surgical visits, including preoperative evaluation, consultation, postoperative care, and long-term follow-up.6–14 The COVID-19 pandemic resulted in worldwide implementation of practices designed to limit the spread of SARS-CoV-2, including the transition of many necessary interactions to electronic and telecommunications. The initial guidelines from governmental and professional organizations prompted hospitals to cancel elective surgeries; however, emergency surgical care and surgical management of time-sensitive conditions required ongoing consultation and patient evaluation. To minimize both staff and patient exposure to infected individuals, many surgical assessments shifted to electronic and telecommunications platforms. This was a new process in many practices and, while various guidelines and recommendations have been published, data on the perceived effectiveness and surgical patients’ experience are lacking.15–30
In this study, we sought to evaluate patients’ experience with newly implemented colorectal and head and neck surgery telemedicine practices at an academic, tertiary care facility during the COVID-19 era. Surveys were administered to patients in the department of surgery to gauge patients’ experience with telemedicine visits. The importance of this finding is that surgical preoperative consultation, postoperative follow-up, and routine visits can be conducted primarily via telemedicine with the benefit of improved communication, lower cost to patients, and avoiding potential opportunities for viral exposure.
This was an observational study conducted in academic surgical subspecialty practices at a tertiary care facility. Institutional Review Board (IRB) approval was granted for the study before data collection. Following COVID-19 pandemic precautions, both the Division of Otolaryngology-Neurotology and the Division of Colon and Rectal Surgery transitioned to telemedicine conducted via telephone or Electronic medical records (EMR)-based video software for the majority of clinic visits. This included initial patient consultations, preoperative appointments, postoperative follow-up visits, and long-term follow-up. Selected patients who required physical examination or minor procedures (e.g., suture removal) maintained traditional in-office visits.
Patients of 18 years age and older in the Division of Otolaryngology-Neurotology or the Division of Colon and Rectal Surgery were eligible to participate. Data were collected from March to June 2020 after COVID-19 protocols were implemented at our institution. Patients were defined as being high risk according to the Center for Disease Control (CDC) guidelines, which included patients of age 65 years or above, living in a nursing home or long-term care facility, being in an immunocompromised state, or having a chronic illness.
Each patient was invited by email to fill out a 66-question survey constructed using an online survey-building platform (Qualtrics, Provo, UT) to assess their experience with the telemedicine or in-office visit. The survey was adapted from previously published TeleENT Satisfaction Questionnaire and Medical Communication Competence Scale (MCCS).31,32 Patients who completed traditional in-office visits during this time were sent only the MCCS to serve as a control. Responses were based on a Likert scale of 1 to 7. Medical Communication Competence Scale responses were pooled according to the four clusters proposed by Cegala et al., which included the following domains: information giving, information seeking, information verifying, and socioemotional communication.32
Data analysis was performed using an online survey platform (Qualtrics, Provo, UT) and IBM SPSS Statistics for Windows, Version 26 (IBM Corp., Armonk, NY). Normally distributed data are described using the mean and standard deviation. Specifically, Likert responses are described using the mean rather than the median to better reflect the trend in responses. Categorical data are described by frequencies and proportions. Comparisons between categorical variables were carried out with the chi-square test. Continuous variables were compared with student’s t-test for two categories. We considered results to be statistically significant if the probability value was less than or equal to 0.05.
The total number of respondents was 74, with an overall response rate of 15.4% (Table 1). Twenty-two surveys were returned from patients evaluated in the Division of Colon and Rectal Surgery out of the 186 eligible patients who were sent the survey (response rate = 11.8%). In total, 52 surveys (25 telemedicine and 27 in-office controls) were returned from patients of the Division of Otolaryngology-Neurotology out of 293 surveys sent, yielding a response rate of 17.7%. The average respondent was 50.5 years old. Forty-nine percent of respondents identified themselves as part of an at-risk population for COVID-19 infection according to CDC guidelines.
Table 1. Patient demographics
| Characteristics | Total (n = 74) |
|---|---|
| Telehealth Colorectal ENT In-office control |
47 (63.5%) 22 (46.8%) 25 (53.2%) 27 (36.5%) |
| Mean age ± standard deviation | 50.5 ± 17.4 years |
| Education No high school High school Associate degree Bachelor’s degree Graduate school |
6 (2.8%) 13 (22.9%) 14 (18.9%) 22 (29.7%) 19 (25.7%) |
Survey respondents felt that telemedicine worked well as a medium for delivering health care and were satisfied with the care that they received (mean Likert 6.19/7) (Table 2). Participants felt that there were several advantages of telemedicine over traditional in-office visits, including requiring less time off from work (mean Likert 5.87/7), the visit itself taking less time (76.6% of respondents), and saving money (83% of respondents) ranging from $3 to $2,000 (mean $108.70 ± $374.14). Ninety-one percent of respondents agreed that utilizing telemedicine allowed them to avoid exposure to the SARS-CoV-2 virus during the COVID-19 pandemic. Eleven patients (23.4%) in the telemedicine cohort expressed a preference for telemedicine visits in the future for routine care, postoperative follow-up and initial consultation. Ninety-six percent of patients would use telemedicine services again if given the option.
Table 2. Telemedicine experience
| Questions | Responses (n = 47) |
|---|---|
| Would you be comfortable going to the doctor’s office for a telemedicine encounter? Yes No |
29 (61.7%) 18 (38.3%) |
| Do you believe that the encounter took more or less time due to the use of telemedicine? Significantly more time More time Same amount of time Less time Significantly less time |
0 1 (2.1%) 10 (21.3%) 22 (46.8%) 14 (29.8%) |
| I am conducting my telemedicine visit on the following device: Laptop/desktop computer Smartphone Tablet |
4 (8.5%) 34 (72.3%) 9 (19.1%) |
| Obtaining the electronic device to use for this telemedicine visit was: Easy Average difficulty Hard |
41 (87.2%) 5 (10.6%) 1 (2.1%) |
| Setting up this telemedicine encounter was: Easy Average difficulty Hard |
38 (80.9%) 7 (14.9%) 2 (4.3%) |
| Has the use of a telehealth encounter rather than a face-to-face encounter saved you money when acquiring care? Yes No |
39 (83.0%) 8 (17.0%) |
| Estimate the amount of money saved: Less than $20 $20–$100 Greater than $100 No response |
19 (40.4%) 8 (17.1%) 5 (10.6%) 15 (31.9%) |
| I am part of an at-risk population for infection with COVID-19 according to the CDC definition. * Yes No |
23 (48.9%) 24 (51.1%) |
*CDC definition: Age 65 or over, living in a nursing home or long-term care facility, being in an immunocompromised state, or having a chronic illness.
The majority of participants utilized smartphones for their appointments (72.3%), though several respondents provided feedback that they would have preferred to use a desktop or laptop computer. Ninety-six percent of respondents reported that setting up the encounter was no more than “average” difficulty (Likert 4/7), with 81% noting that the process was easy. Ninety-eight percent of patients stated that obtaining the device used for the encounter was no more than “average” difficulty, with one respondent (2.13%) reporting that it was difficult to obtain the device.
Thirty-six percent of respondents at least somewhat agreed that the quality of care was hindered by the lack of a physical examination (Table 3). Sixty-two percent at least somewhat agreed that they would prefer a face-to-face appointment rather than a telemedicine consultation. These patients remarked that telemedicine visits felt less personal, they felt less connection with their physician, and they felt that there was part of their evaluation that might have been missed due to the lack of physical examination (Supp. Table 1). However, most respondents felt that the telemedicine visit met their expectations for a doctor’s appointment (87.2% at least somewhat agreed).
Table 3. Colorectal versus ENT telemedicine-specific questions
| Questions | ENT average Likert score (n = 25) | Colorectal average Likert score (n = 22) | p-value |
|---|---|---|---|
| I could see the doctor clearly during the telemedicine visit (for video visits). | 5.5 ± 2.2 | 6.82 ± 0.4 | 0.01* |
| I had no trouble hearing the doctor when he or she spoke to me. | 5.73 ± 1.6 | 6.64 ± 0.7 | 0.01* |
| The doctor seemed to understand my problem. | 6.59 ± 0.7 | 6.86 ± 0.4 | 0.08 |
| I was comfortable with and understood what the doctor told me about my complaint. | 6.23 ± 1.5 | 6.45 ± 1.4 | 0.63 |
| A telemedicine visit makes receiving care more accessible (i.e., I don’t have to drive as far or wait as long to get an appointment). | 6.18 ± 1.3 | 6.27 ± 1.0 | 0.82 |
| Telemedicine saves me time traveling to a hospital or specialty clinic. | 6.55 ± 0.6 | 6.55 ± 0.9 | 1 |
| I needed less time off work for the telemedicine visit compared with an in-person visit. | 6 ± 1.3 | 5.86 ± 1.5 | 0.65 |
| I find telemedicine an acceptable way to receive medical services. | 5.5 ± 1.1 | 5.86 ± 1.2 | 0.29 |
| I would prefer a face-to-face visit with a specialist rather than a telemedicine consultation. | 4.73 ± 1.1 | 4.27 ± 2.1 | 0.29 |
| This telemedicine visit was as good as a face-to-face encounter. | 4.91 ± 1.4 | 4.91 ± 1.5 | 1 |
| Overall, I am satisfied with the quality of service being provided via telemedicine. | 6 ± 1.2 | 6.41 ± 0.6 | 0.10 |
| I would use telemedicine services again. | 6.18 ±0.8 | 6.32 ± 0.8 | 0.56 |
| The quality of care delivered was hindered by the doctor not being able to perform a physical exam on me during this visit. | 3.77 ± 1.5 | 3.55 ± 1.9 | 0.70 |
| The telemedicine encounter met my expectations for a visit with my physician. | 5.36 ± 1.3 | 6.14 ± 1.0 | 0.03* |
*Value is statistically significant, p < 0.05.
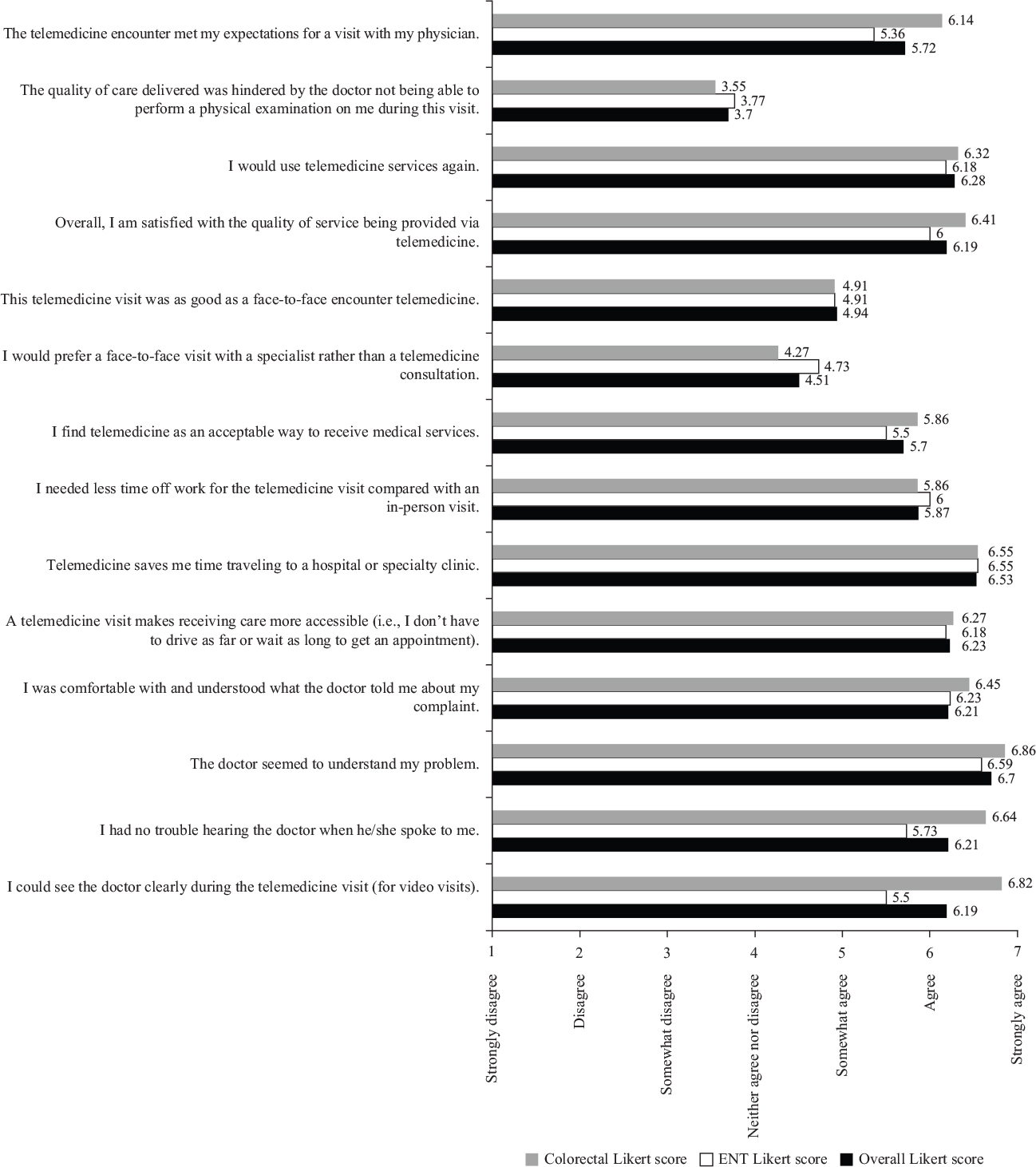
Among the telemedicine population, the colorectal cohort had a significantly easier time seeing and hearing the doctor with the video interface when compared with the ear, nose and throat (ENT) cohort ( p = 0.007 and p = 0.008, respectively) (Table 3). The colorectal patients undergoing telehealth appointments were significantly more likely to rate their telemedicine encounter as meeting their expectations for a visit with their physician ( p = 0.031). All other telemedicine components measured were not significantly different between the two cohorts (Figure 1).
Figure 1—Likert scale for telemedicine-specific questions.
When comparing the combined telehealth cohort with the in-office control appointments, the telehealth cohort scored significantly higher ( p < 0.05) for questions corresponding to the following domains: patient’s competence in information giving, patient’s competence in information verifying, patient’s competence in information seeking, doctor’s competence in information giving, and doctor’s competence in socioemotional communication (Table 4). There were no significant differences between the two cohorts corresponding to the domains: patient’s competence in socioemotional communication ( p = 0.12), doctor’s competence in information verification ( p = 0.19), and doctor’s competence in information seeking ( p = 0.41).
Table 4. Telehealth versus in-office visit Medical Communication Competence Scale (MCCS) clusters
| Questions | Telehealth average Likert score (n = 47) | In-office average Likert score (n = 27) | p-value |
|---|---|---|---|
| Patient’s competence in information giving | 6.56 ± 0.20 | 5.86 ± 0.16 | <0.01* |
| Patient’s competence in information verifying | 6.50 ± 0.10 | 5.83 ± 0.15 | <0.01* |
| Patient’s competence in information seeking | 6.39 ± 0.14 | 5.64 ± 0.14 | 0.01* |
| Patient’s competence in socioemotional communication | 6.73 ± 0.12 | 5.94 ± 0.08 | 0.12 |
| Doctor’s competence in information giving | 6.05 ± 0.59 | 5.56 ± 0.55 | <0.01* |
| Doctor’s competence in information verifying | 6.40 ± 0.11 | 6.32 ± 0.05 | 0.19 |
| Doctor’s competence in information seeking | 6.51 ± 0.09 | 6.60 ± 0.15 | 0.41 |
| Doctor’s competence in socioemotional communication | 6.58 ± 0.11 | 6.75 ± 0.13 | 0.01* |
*Value is statistically significant, p < 0.05.
The COVID-19 pandemic resulted in drastic changes to the way that physicians can practice medicine. Limiting the spread of the virus and allocation of scarce health care resources required major alterations in the delivery of health care in both inpatient and outpatient settings. Recommendations from the American College of Surgeons suggested that health systems, hospitals, and surgeons “review all scheduled elective procedures with a plan to minimize, postpone, or cancel electively scheduled operations.”33 Similar guidelines and recommendations were made by national and global health organizations.
One recommendation of the health care-governing agencies was the increased use of telemedicine.29 For most practices, this involved expansion or novel implementation of telemedicine visits. In particular, surgical care has been slower to adopt telemedicine as many surgical fields rely on physical examination techniques for diagnosis. Many of these physical examination maneuvers cannot be adapted to a telemedicine visit with a patient in a non-clinical setting. To circumvent this problem, some smartphone applications have been created to help assess vital signs and lung function. With respect to otolaryngology, we adapted an on-line smartphone app to assess a patient’s hearing prior to the visit (Hearingtest.online). In situations where the chief complaint was otalgia, several questions related to ear pain, drainage, associated hearing loss, and the patient’s self-examination of their jaw joint for pain and crepitus easily led to a diagnosis. Other patients with a presenting symptom of sudden deafness were instructed to use an app to perform a Weber test using iBrateMe! (Vmlweb LTD.)34 However, many surgical subspecialties utilize procedures that are not replicable over a telemedicine encounter, including otoscopic examination, laryngoscopy, digital rectal examination, and anoscopy. This may be even more pronounced in otolaryngology, as many patients in this cohort remarked on the lack of otoscopic examination as a drawback of telemedicine. These patients were significantly less likely to state that the telemedicine visit met their expectations for a doctor’s appointment than the colorectal patients (Table 3). In addition, there may be additional difficulties utilizing telemedicine for those with hearing pathology as colorectal patients had less difficulty hearing and seeing the physician during the telemedicine appointment when compared with the otolaryngology cohort. This might be due to the handicap that these patients experience and the limitations in technology to reflect the audiovisual cues on which hearing loss patients rely.
While the technological limitations of telemedicine visits were reflected in our patient-survey results, the majority of patients were satisfied with the care that they received (Table 3). It is possible that this is a direct result of the COVID-19 pandemic and patients’ reluctance to enter a traditional health care setting despite preferring face-to-face visits and that their satisfaction carries an implied, “under the circumstances.” However, patient satisfaction has been similarly high and equivalent or superior to office visits in pre-COVID studies performed by Buvik et al., Goedeke et al., and Viers et al.3,35,36 Interestingly, Goedeke et al. also found that patients felt the quality of interaction was superior for telemedicine visits.36 This is similar to our results, in which the telehealth cohort scored significantly higher on the MCCS when compared with the in-office controls with the patients’ perceived ability to give, verify, and seek information from the doctor and the doctor’s ability to give information and engage in socioemotional communication (Table 4). With this better-perceived communication, patients may feel they can better express their symptoms and gather information from the doctor regarding their diagnosis. These results may indicate that telemedicine patients felt more focused when discussing their symptoms and diagnosis and that the doctors’ ability to convey their support for the patient was improved compared with in-person visits. Despite patients’ concern that they were not able to connect with their physician as easily during a telehealth visit, most of these patients felt that their appointment met or exceeded expectations for a doctors’ visit and would use telemedicine services in the future if offered (Supp. Table 2). This demonstrates that, while patients acknowledge the limitations of telemedicine and might even be more concerned than providers about this impacting their care, they perceive value in some of the advantages offered and can envision ways in which they would like to use it.
Several patients indicated a preference for telemedicine over traditional office visits when feasible, particularly for follow-up appointments (Supp. Table 1). This was also seen in the study by Safir et al., in which 98% of patients indicated a preference for telephone-based encounters over in-person clinical visits and that by Buvik et al. in which 86% of patients who had an initial video-based consultation would prefer such visits in the future.6,35 These findings suggest that initial consultation and routine care are potential forums for expanding telemedicine use in surgery beyond the COVID-19 pandemic. In addition, many patients had a complete surgical evaluation remotely with physical examination delayed until the day of surgery. These findings should not diminish the value of in-person interaction for building rapport, non-verbal communication, or essential examination maneuvers or procedures. However, they highlight the potential utility of telemedicine to provide expert specialty evaluation to patients whose geographic location (e.g., in a rural, remote area), financial or temporal limitations, family responsibilities, or other situations might prevent access to this care.
Telemedicine visits are convenient and easily arranged as smart devices have become nearly ubiquitous (91.4% of respondents conducted their visit via smartphone or tablet). Most respondents had little or no difficulty acquiring the appropriate device and setting up their appointment. For patients who struggle to obtain or use the necessary equipment, a telemedicine visit with a distant specialist may also be arranged through the patient’s primary care physician or other local clinics.31 This broadens access to patients who lack the socioeconomic means or technological skills to purchase and operate a smart device or computer and internet access. Sixty-two percent of respondents in our survey said they would be comfortable going to a doctor’s office for a telemedicine visit.
Because of the circumstances surrounding the implementation of telemedicine visits at our institution, we included all types of surgical clinic visits in our study. This includes initial consultation, additional preoperative evaluation, signing of consent forms, postoperative visits, and long-term follow-up. Prior publications studied the application of telemedicine to a single visit type and focused primarily on postoperative care.3,5,37–41,42 As the transition to telemedicine visits was not voluntary for patients at our institution during the COVID-19 pandemic, the study population is not biased either toward or against virtual interactions, whereas many other studies required patients to “opt-in” to the telemedicine program. This study has good external validity regarding the ability of patients to obtain a suitable device and set up the telemedicine visit as devices or training to conduct the appointment were not supplied to patients in this study.
Our study has several limitations. The overall response rate was low at 15.4%; therefore, our results are subject to nonresponse bias, which may limit the generalizability of our results. This low response rate is likely multifactorial but may at least be partially attributable to survey fatigue due to a large number of questions and the repetitiveness of the MCCS in particular, to patient reluctance to spend additional time on electronic devices when many had shifted to remote work, to forgotten surveys as we sent a single reminder email, or to a lack of incentivization for the response. The study population was limited to patients in the Division of Otolaryngology or the Division of Colon and Rectal Surgery at a single academic medical center, so our results may not be applicable to all surgical populations. In addition, although we perceived some advantages to including patients with a broad range of visit types, we did not include a means of comparing responses between visit types. This would be a valuable component to include in future studies, as the limitations of evaluation (or at least patient-perceived limits) via telemedicine will have a different impact on a new patient evaluation compared with postoperative or long-term follow-up. Our data quality is also limited by the observational nature of this study. While a randomized trial was not feasible with the restrictions related to the pandemic limiting in-person visits, this introduces bias that particularly affects our comparisons between those visits and telemedicine visits (i.e., there are likely differences in patients who received in-office visits during that time and those who had telephone or video encounters). No data were gathered on how many telemedicine patients required additional in-person evaluation prior to surgery. For these patients, the benefits of having an initial telemedicine visit should be analyzed in future studies.
While we believe that our experience provides insight into the promise and challenges of rapidly initiating or scaling up a surgical telemedicine program in the COVID era, long-term results through multiple iterations and development of these programs will allow for more specific recommendations. In addition, larger, multicenter trials would allow for greater generalizability of the results. It will also be important to reevaluate programs that are established during the pandemic to ensure that they are still able to meet the needs of patients and providers in the future.
The COVID-19 pandemic resulted in a widespread transition of traditional in-office visits to telephone and EMR-based video visits. While the majority of respondents preferred face-to-face visits, most patients were satisfied with the care they received via telemedicine. The telemedicine patients experienced an improved ability to communicate their symptoms to the doctor and gather information regarding their visit. These patients noticed that the telemedicine encounters met their expectations for a doctors’ appointment, were easy to arrange, saved both time and money, and kept them safe from potential exposure during the COVID-19 pandemic. In the light of a second wave of infections or the possibility of future infectious disease outbreaks, our results suggest that telemedicine may keep both patients and providers safe from exposure while providing satisfactory surgical care at all stages of evaluation.
Funding statement: The authors did not receive funding or support for this project.
Conflicts of Interest: There are no conflicts of interest to disclose.
Contributors: All authors contributed to the design and implementation of the research, analysis of the results, and writing of the manuscript.
Acknowledgments: The authors wish to acknowledge Drs Nicole Lopez, Samuel Eisenstein, Bard Cosman, Lisa Perry, and Benjamin Abbadessa for their assistance in data acquisition.
| 1. | Model Policy for The Appropriate Use of Telemedicine Technologies in the Practice of Medicine. FSMB; 2014 [cited 2020 Jun 8]. Available from: https://www.fsmb.org/siteassets/advocacy/policies/fsmb_telemedicine_policy.pdf |
| 2. | Mobile fact sheet. Pew Research Center; 2019 [cited 2020 Jun 8]. Available from: https://www.pewresearch.org/internet/fact-sheet/mobile/ |
| 3. | Viers BR, Lightner DJ, Rivera ME, et al. Efficiency, satisfaction, and costs for remote video visits following radical prostatectomy: A randomized controlled trial. Eur Urol. 2015;68(4):729–35. https://doi.org/10.1016/j.eururo.2015.04.002 |
| 4. | Holt B, Faraklas I, Theurer L, et al. Telemedicine use among burn centers in the United States: A survey. J Burn Care Res. 2012;33(1):157–62. https://doi.org/10.1097/BCR.0b013e31823d0b68 |
| 5. | Gunter RL, Chouinard S, Fernandes-Taylor S, et al. Current use of telemedicine for post-discharge surgical care: A systematic review. J Am Coll Surg. 2016;222(5):915–27. https://doi.org/10.1016/j.jamcollsurg.2016.01.062 |
| 6. | Safir IJ, Gabale S, David SA, et al. Implementation of a tele-urology program for outpatient hematuria referrals: Initial results and patient satisfaction. Urology. 2016;97:33–9. https://doi.org/10.1016/j.urology.2016.04.066 |
| 7. | Cain SM, Moore R, Sturm L, et al. Clinical assessment and management of general surgery patients via synchronous telehealth. J Telemed Telecare. 2017;23(2):371–5. https://doi.org/10.1177/1357633X16636245 |
| 8. | Jue JS, Spector SA, Spector SA. Telemedicine broadening access to care for complex cases. J Surg Res. 2017;220:164–70. https://doi.org/10.1016/j.jss.2017.06.085 |
| 9. | Valsangkar NP, Eppstein AC, Lawson RA, Taylor AN. Effect of lean processes on surgical wait times and efficiency in a tertiary care veterans affairs medical center. JAMA Surg. 2017;152(1):42–7. https://doi.org/10.1001/jamasurg.2016.2808 |
| 10. | Dean P, O’Donnell M, Zhou L, Skarsgard ED. Improving value and access to specialty medical care for families: A pediatric surgery telehealth program. Can J Surg. 2019;62(6):436–41. https://doi.org/10.1503/cjs.005919 |
| 11. | Asiri A, AlBishi S, AlMadani W, et al. The use of telemedicine in surgical care: A systematic review. Acta Inform Med. 2018;26(3):201–6. https://doi.org/10.5455/aim.2018.26.201-206 |
| 12. | Mullen-Fortino M, Rising KL, Duckworth J, et al. Presurgical assessment using telemedicine technology: Impact on efficiency, effectiveness, and patient experience of care. Telemed J E Health. 2019;25(2):137–42. https://doi.org/10.1089/tmj.2017.0133 |
| 13. | Paquette S, Lin JC. Outpatient telemedicine program in vascular surgery reduces patient travel time, cost, and environmental pollutant emissions. Ann Vasc Surg. 2019;59:167–72. https://doi.org/10.1016/j.avsg.2019.01.021 |
| 14. | Schroeder C. Pilot study of telemedicine for the initial evaluation of general surgery patients in the clinic and hospitalized settings. Surg Open Sci. 2019;1(2):97–9. https://doi.org/10.1016/j.sopen.2019.06.005 |
| 15. | Catanese S, Pentheroudakis G, Douillard JY, Lordick F. ESMO Management and treatment adapted recommendations in the COVID-19 era: Pancreatic cancer. ESMO Open. 2020;5(Suppl 3). https://doi.org/10.1136/esmoopen-2020-000804 |
| 16. | Contreras CM, Metzger GA, Beane JD, et al. Telemedicine: Patient-provider clinical engagement during the COVID-19 pandemic and beyond. J Gastrointest Surg. 2020:1–6. https://doi.org/10.1007/s11605-020-04623-5 |
| 17. | Grenda TR, Whang S, Evans NR. Transitioning a surgery practice to telehealth during COVID-19. Ann Surg. 2020. https://doi.org/10.1097/SLA.0000000000004008 |
| 18. | Hakim AA, Kellish AS, Atabek U, et al. Implications for the use of telehealth in surgical patients during the COVID-19 pandemic. Am J Surg. 2020. https://doi.org/10.1016/j.amjsurg.2020.04.026 |
| 19. | Hemingway JF, Singh N, Starnes BW. Emerging practice patterns in vascular surgery during the COVID-19 pandemic. J Vasc Surg. 2020. https://doi.org/10.1016/j.jvs.2020.04.492 |
| 20. | Kling SM, Philp MM. The effects of the COVID-19 pandemic on oncological surgery. J Surg Case Rep. 2020;5. https://doi.org/10.1093/jscr/rjaa157 |
| 21. | Latifi R, Doarn CR. Perspective on COVID-19: Finally, telemedicine at center stage. Telemed J E Health. 2020. https://doi.org/10.1089/tmj.2020.0132 |
| 22. | Layfield E, Triantafillou V, Prasad A, et al. Telemedicine for head and neck ambulatory visits during COVID-19: Evaluating usability and patient satisfaction. Head Neck. 2020. https://doi.org/10.1002/hed.26285 |
| 23. | Mascagni D, Eberspacher C, Mascagni P, et al. From high volume to “zero” proctology: Italian experience in the COVID era. Int J Colorectal Dis. 2020:1–4. https://doi.org/10.1007/s00384-020-03622-x |
| 24. | Pignatti M, Pinto V, Miralles MEL, et al. How the COVID-19 pandemic changed the Plastic Surgery activity in a regional referral center in Northern Italy. J Plast Reconstr Aesthet Surg. 2020. https://doi.org/10.1016/j.bjps.2020.05.002 |
| 25. | Plocienniczak MJ, Noordzij JP, Grillone G, et al. Guidelines for resident participation in otolaryngology telehealth clinics during the COVID-19 pandemic. Otolaryngol Head Neck Surg. 2020. https://doi.org/10.1177/0194599820932133 |
| 26. | Shipchandler TZ, Nesemeier BR, Parker NP, et al. Telehealth opportunities for the otolaryngologist: A silver lining during the COVID-19 pandemic. Otolaryngol Head Neck Surg. 2020. https://doi.org/10.1177/0194599820929641 |
| 27. | Shirke MM, Shaikh SA, Harky A. Tele-oncology in the COVID-19 era: The way forward? Trends Cancer. 2020. https://doi.org/10.1016/j.trecan.2020.05.013 |
| 28. | Tanaka MJ, Oh LS, Martin SD, Berkson EM. Telemedicine in the era of COVID-19: The virtual orthopaedic examination. J Bone Joint Surg Am. 2020. https://doi.org/10.2106/JBJS.20.00609 |
| 29. | Vecchione L, Stintzing S, Pentheroudakis G, et al. ESMO management and treatment adapted recommendations in the COVID-19 era: Colorectal cancer. ESMO Open. 2020;5. https://doi.org/10.1136/esmoopen-2020-000826 |
| 30. | Walędziak M, Różańska-Walędziak A, Pędziwiatr M, et al. Bariatric surgery during covid-19 pandemic from patients’ point of view-the results of a national survey. J Clin Med. 2020;9(6). https://doi.org/10.3390/jcm9061697 |
| 31. | Seim NB, Philips RHW, Matrka LA, et al. Developing a synchronous otolaryngology telemedicine clinic: Prospective study to assess fidelity and diagnostic concordance. Laryngoscope. 2018;128(5):1068–74. https://doi.org/10.1002/lary.26929 |
| 32. | Cegala DJ, Coleman MT, Turner JW. The development and partial assessment of the medical communication competence scale. Health Commun. 1998;10(3):261–88. https://doi.org/10.1207/s15327027hc1003_5 |
| 33. | American College of Surgeons. COVID-19: Recommendations for management of elective surgical procedures 2020. [cited 2020 Jun 15]. Available from: https://www.facs.org/covid-19/clinical-guidance/elective-surgery |
| 34. | Ungar OJ, Handzel O, Cavel O, Oron Y. A smartphone-based weber test may discriminate between a conductive and a sensorineural hearing loss. Audiol Neurotol. 2019;24(4):191–6. https://doi.org/10.1159/000502274 |
| 35. | Buvik A, Bugge E, Knutsen G, et al. Patient reported outcomes with remote orthopaedic consultations by telemedicine: A randomised controlled trial. J Telemed Telecare. 2019;25(8):451–9. https://doi.org/10.1177/1357633X18783921 |
| 36. | Goedeke J, Ertl A, Zöller D, et al. Telemedicine for pediatric surgical outpatient follow-up: A prospective, randomized single-center trial. J Pediatr Surg. 2019;54(1):200–7. https://doi.org/10.1016/j.jpedsurg.2018.10.014 |
| 37. | Hwa K, Wren SM. Telehealth follow-up in lieu of postoperative clinic visit for ambulatory surgery: Results of a pilot program. JAMA Surg. 2013;148(9):823–7. https://doi.org/10.1001/jamasurg.2013.2672 |
| 38. | Kummerow BK, Roumie CL, Stewart MK, et al. Implementation of a telephone postoperative clinic in an integrated health system. J Am Coll Surg. 2016;223(4):644–51. https://doi.org/10.1016/j.jamcollsurg.2016.07.010 |
| 39. | Nikolian VC, Williams AM, Jacobs BN, et al. Pilot study to evaluate the safety, feasibility, and financial implications of a postoperative telemedicine program. Ann Surg. 2018;268(4):700–7. https://doi.org/10.1097/SLA.0000000000002931 |
| 40. | Soegaard Ballester JM, Scott MF, Owei L, et al. Patient preference for time-saving telehealth postoperative visits after routine surgery in an urban setting. Surgery. 2018;163(4):672–9. https://doi.org/10.1016/j.surg.2017.08.015 |
| 41. | Williams AM, Bhatti UF, Alam HB, Nikolian VC. The role of telemedicine in postoperative care. Mhealth. 2018;4:11. https://doi.org/10.21037/mhealth.2018.04.03 |
| 42. | Shapiro SB, Lipschitz N, Kemper N, et al. Early experience with telemedicine in patients undergoing otologic/neurotologic procedures. Otol Neurotol. 2020. https://doi.org/10.1097/MAO.0000000000002774 |
Table S1. Telemedicine comments
| Category | Patient’s comments |
|---|---|
| Physician’s time management | Appears to give better management of time for the doctor with caseload. The doctor was the ultimate professional in our teleconference. The added bonus was that the screen was split, and her nurse and office manager also participated. I received the full attention of the doctor’s clinical perceptions, just less the added advantage of physical presentation. I thought it was efficient and great; however, I have a fantastic doctor, and he made the most of the appointment. |
| Patient’s time management | I live mostly in Los Angeles, so telehealth helps me to keep my medical care team without frequent trips to San Diego. It saved a lot of traveling and time also paying people for gas if my transportation didn’t go through, I have to find rides this helps a lot. It saved time driving not having to drive to San Diego. It’s easier for me since I live 2+ hours away and any travel is difficult It’s efficient in time and cost My visit was very short as was expected. It was really nice to not have to drive the 45 minutes it would have taken me to get there, and to not have to pay for parking. This is a huge time and money saver since I live 40+ miles from UCSD. Saves me from a long drive, gas, and parking This would have been an out of state visit for me. I live in Oregon and am seeking specialty surgical treatment. Much easier this way for initial consults. |
| COVID-19 specific | Feel safer not leaving home Less risk to be exposed to COVID-19 Less travel expenses, easier access to appointments and medical information/records through an app, and lowering the risk for disease exposure (COVID-19) Saves money, time, and unnecessary potentially exposure to COVID-19 The benefits are unique to the risks imposed on society by the COVID-19 virus. |
| Beneficial for follow-up visits | For many routine appointments I’d prefer telemedicine appointments just for the time savings. Great for discussions that don’t require in person testing. I believe that it was beneficial and should be used more often moving forward. However, there are certain situations that do require a face-to-face visit that should not be replaced. I would like to do all my appointments this way that I can If you don’t have a need for a physical exam, teleconferencing is the way to go. It allowed me to be more comfortable after my surgery and that I didn’t have to travel. It was a nice alternative when a physical evaluation isn’t needed but instructions and information need to be relayed to patients. |
| Beneficial for follow-up visits | It was helpful to have the doctor’s extensive knowledge of ENT. I would be more confident in the diagnosis if they had been able to look in my ear or touch me if necessary, to help in the diagnosis. Telehealth visit is great if I don’t need a physical exam. I usually need the physical examination. Telehealth will be useful for consultations, with a face-to-face visit used when necessary. This was a follow-up visit, so no issues or special comments. I have no concerns. It’s a great alternative to in-office visits that don’t involve a physical examination. |
Table S2. Telemedicine concerns
| Category | Patient’s concerns |
|---|---|
| Desire for a physical examination | Certain situations require a physical examination. Checking eye function for my double vision I don’t get my vitals taken or my lungs listened to in telemedicine Sometime doctors need to have a better look at the problem, for example, I feel it would’ve been better to have the doctor take a look at my eardrum in person. Telehealth visit is great if I don’t need a physical examination. I usually need the physical examination. If you don’t have a need for a physical examination, teleconferencing is the way to go. I have no concerns. It’s a great alternative to in-office visits that don’t involve a physical examination. Telehealth is acceptable if there is not a need for physical examination. In my case I needed to repeat the appointment with a face-to-face encounter because there was a need for a physical examination. In that case I had to pay for both appointments, which means it cost me double. However, the telehealth was my choice since the health issue was urgent and worrisome and took place during a time when I was unwilling to come to a hospital. It was helpful to have the doctor’s extensive knowledge of ENT. I would be more confident in the diagnosis if they had been able to look in my ear or touch me if necessary, to help in the diagnosis. Without the examination, the doctor does not seem to be receiving enough information to diagnose the patient. |
| Device/connectivity problems | Connection issues/device accessibility since the telehealth visit must be conducted on an app—for those who have poor internet connections or lack access to a “smart device.” |
| Patient–physician interaction | I missed getting a hug from my doctor. Less non-verbal interaction (body language, tonal inflection, facial expressions), so not as “complete” a connection as when meeting in person. Lose a little flow/back and forth that may lead to wider ranging discussion. There is almost always less personal satisfaction without face-to-face interaction. |
| Need for face-to-face visit or in-person tests | Great for discussions that don’t require in-person testing. I believe that it was beneficial and should be used more often moving forward. However, there are certain situations that do require a face-to-face visit that should not be replaced. |
Copyright Ownership: This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, adapt, enhance this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0.