ORIGINAL CLINICAL RESEARCH
A Tale of Two Counties with the Same Telehealth Story: Experience with Cancer Genetics Testing During Covid-19 at a Community Hospital
Allison Jay, MD1* , Hannah Kelley, BS2 and M. Susan Jay, MD3
, Hannah Kelley, BS2 and M. Susan Jay, MD3
1Division of Cancer Genetics, Ascension St. John Hospital, Detroit, Michigan, USA; 2NateraTM Austin, Texas, USA; 3Division of Adolescent Medicine, Department of Pediatrics, Medical College of Wisconsin, Milwaukee, Wisconsin, USA
Keywords: cancer, community health, genetics, patient engagement, urban health
Abstract
Introduction: With the onset of the COVID-19 pandemic in 2020, telemedicine offered providers an alternative diagnostic and treatment resource in many areas of medicine, including oncology and cancer genetics. This care option, paired with the ability of genetic testing labs to send saliva-based DNA collection kits to patients, enabled our community hospital in Detroit, Michigan, USA, to offer diagnostic testing without requiring patients to travel to a healthcare setting for a host of reasons. Social determinants of health influence success with telehealth, and this study sought to analyze how successful telehealth cancer genetics care was throughout the Detroit Metropolitan area.
Methods: Patient demographics for in-person visits 6 months before COVID were analyzed, then compared with patients’ demographics during the 2020–2021 pandemic using telehealth, and 7 months after the pandemic’s peak.
Results: Pre-COVID, 192 unique patients were seen in person, with the top three cities of patients being Detroit (12.1%), Clinton Township (8.3%), and Saint Clair Shores (10.4%). During the pandemic, with telehealth as the primary modality, the top three cities were Macomb (7.2%), Detroit (7%), and Clinton Township (7%). Seven months of post-pandemic period were analyzed. There were 176 patients seen, with the top cities being Saint Clair Shores (6.8%) and the cities of Macomb, Detroit, and Clinton Township equivalent (4.5%). Because demographic data were more readily available for counties, we examined these in greater detail. Detroit is in Wayne County, while St. Clair Shores, Macomb, and Clinton Township are in Macomb County. As per the United States Census Bureau, Macomb County has a median income of $64,641, while Wayne County has a median income of $49,359. The poverty level in Macomb County is 9.2%, whereas, in Wayne County, the poverty level is 20%.
Conclusions: This article outlines the challenges of initiating a telemedicine program in an urban community area and highlights the benefits of a concierge service for cancer patients who may have economic and historically poor perceived technological abilities.
Citation: Telehealth and Medicine Today © 2023, 8: 382 - http://dx.doi.org/10.30953/tmt.v8.382
Copyright: © 2023 The Authors. This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, adapt, enhance this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0.
Received: November 28, 2022; Accepted: December 20, 2022; Published: April 24, 2023
Competing interests and funding: Allison M. Jay had no financial/non-financial relationships. M. Susan Jay had no financial relationships/non-financial relationships. Hannah Kelley previously worked at Ascension during the course of data collection, and now works at Natera, a genetic testing company.
This study received no funding.
No financial disclosures.
*Corresponding Author: Allison Jay, Email: allyjcyprus@hotmail.com
The respiratory disease caused by SARS-CoV-2 (COVID-19) changed how medicine is practiced. In response to the virus, many governors throughout the United States issued stay-at-home orders, which prohibited non-essential in-person work and limited clinical care to those with time-sensitive conditions because of personnel shortages and concern among patients about exposure to infection if already in an immunocompromised state.
With surging infection rates, our community, which included Detroit city and the surrounding metropolitan area, became an epicenter of COVID-19 among vulnerable residents with multiple health ailments, including diabetes, cardiovascular disease, and cancer.1 Social determinants of health include economic stability, education, healthcare access, and neighborhood and social context. As per World Population and Review, Detroit is the most economically disadvantaged city in the United States.2 This study’s goal was to ensure that we maximized access for patients from Detroit so that they could get genetics care during the pandemic, which could impact their cancer treatment.
To continue providing genetics care during the pandemic, our cancer genetics program, with support from the hospital administration, developed a digital platform to conduct telehealth genetics visits during which family history was obtained. Furthermore, patients were counseled about fundamental issues of genetic testing, including its potential impact on other family members. Our program consisted of a genetic assistant and medical geneticist who were transitioned from a brick-and-mortar setting at the outpatient clinical site to a virtual home visit where patients could include family members during their virtual encounter.
With the public health declaration and the COVID public health emergency, three billing policies by the Centers for Medicare and Medicaid (CMS) and private commercial payers were adapted to cover virtual telemedicine and telehealth visits. This enabled patients to continue receiving medical care during the pandemic.3,4 Besides financial concerns, a serendipitous feature offered by genetic testing companies was the option to have DNA saliva collection kits delivered via FedEx to patients, which included prepaid return FedEx labels, so that patients no longer needed to come into the clinic to have blood taken for genetic testing.
Cancer genetics counseling is ideally suited for telemedicine, with each visit focused on discussing information related to familial cancer and inheritable gene changes between the provider and patient. With the patient often in their home environment and without the distraction of preparing for a clinic visit or with additional concerns of weather, parking, and child care, the total focus of the encounter could be on the patient and their history and medical conditions. For example, a 40-year-old mother with breast cancer could now undergo counseling and testing from the safety of her home and learn how genetics might impact getting a lumpectomy versus a bilateral mastectomy for her breast cancer.
The BRCA (BReast CAncer) genes might be the most famous, given actress Angelina Jolie’s publicized personal journey with her mother’s ovarian cancer, published in The New York Times.5 She completed genetic testing and was positive for a BRCA1 mutation associated with up to 44% risk of ovarian cancer and 72% risk of breast cancer. Ms Jolie ultimately decided to do a prophylactic bilateral mastectomy and bilateral salpingo-oophorectomy.
This study sought to evaluate the demographic features of patients in a majority-minority city who were motivated to pursue genetic testing to help their cancer management and also help with cancer surveillance for families.
Materials and Methods
Patients were screened at tumor boards at our community hospital, including in person Breast Tumor Boards, Gastrointestinal Tumor Boards, Urology/Prostate Tumor Boards, and Gynecology/Oncology Tumor boards. Tumor boards transitioned to virtual platforms during the pandemic. Before the pandemic, from September 1, 2010, to February 29, 2020, an electronic medical report was generated using Athena® software with a list of unique patients and zip codes. An Athena® report was also generated for 7 months after the height of the pandemic in 2022. From March 24, 2020, through February 28, 2021, the number of virtual visits was recorded in a log.
At the start of the pandemic, our cancer geneticist and assistant enrolled in the Ascension Online Care/Amwell Platform and completed training on professionalism in telehealth. Two individuals in the group, the geneticist and the genetics assistant, would send patients a link accessible on their computer, Android, or iPhone to prompt the start of each telemedicine appointment. FaceTime, Google Meet, Doximity, or telephone visits were offered for patients who could not access the link. Because of medical/legal concerns and to maintain the security of connections for healthcare discussions, it is best to connect through secure hospital portals/links. Our hospital subsequently instituted a policy to use only the secure hospital portal that offered video links via text message or email. At each “new” patient visit, the geneticist obtained family and personal medical history, counseled the patients on background information related to genetics and cancer, and demonstrated how they would submit their saliva sample.
As previously outlined, the genetic testing companies sent testing kits directly to the patients with a pre-paid return FedEx envelope. The geneticist or genetics assistant scheduled FedEx pickups for all patients and instructed them to leave their packaged sample on the porch at a designated time. After completion of testing, patients were scheduled for a “results” appointment, during which the results were reviewed, and implications for family members were discussed.
Concerning financial considerations before testing, all patients had a benefits investigation and were notified of their out-of-pocket cost for said testing. For actionable/positive genetic results, recommendations were made as per National Cancer Comprehensive Network (NCCN) Guidelines for cancer surveillance/treatment and testing for family members.
The number of patient visits was recorded in a video log that was kept current. The log documented the type of visit (phone or telemedicine), technical difficulties, and whether the patient’s appointment was a new or a return visit. The time spent for each visit and documentation of what was discussed were recorded in the electronic medical record system, Athena®.
This study was reviewed and approved by the IRB Committee and followed the standards of the Declaration of Helsinki.
Results
During the 6 months before the pandemic, 192 unique patients were seen. The top three cities from which patients were from were Detroit (12.1%), Clinton Township (8.3%), and Saint Clair Shores (10.4%) (Figure 1). Detroit is in Wayne County, Clinton Township and Saint Clair Shores are in Macomb County. The top three counties, respectively, were Macomb County (53.1%), Wayne County (31.3%), and Oakland County (7.3%), as outlined in Table 1. Demographics for the top three counties are summarized in Table 2. To give the visualization for locations, see the map in Figure 1.
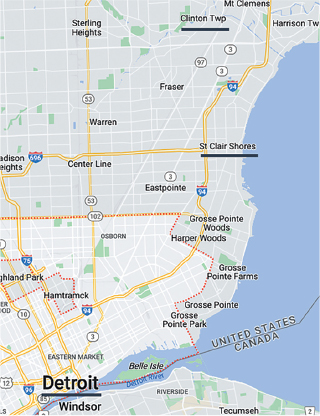
Fig. 1. The top three cities from which patients were drawn included Detroit (12.1%), Clinton Township (8.3%), and Saint Clair Shores (10.4%).
During the pandemic, 528 patients had virtual consultations using telephone or video formats (FaceTime, Google Meet, Doximity, Ascension Video/Chat). Table 1 lists patient percentages of the top three counties for three periods, namely, pre-pandemic, during the pandemic, and post-pandemic. Macomb County, Wayne County, and Oakland County were the top three counties during all three time periods.
Discussion
With the emergence of the COVID-19 pandemic in March 2020, many clinical practices rapidly went virtual via telemedicine within 2–3 weeks. While many patients adopted this new format seamlessly, literature began to emerge regarding those left behind by virtual medicine. In their commentary “The Pandemic of Health Care Inequity,” Thronson et al.6 discuss their local patterns in the Pacific Northwest, which showed a “story of differential access to virtual care.” They report low rates of telemedicine in patients who did not have housing, patients with limited English proficiency, and in a racially diverse population.
Darrat and colleagues also studied the socioeconomic disparities in patient use of telehealth during the pandemic at a tertiary care center in Detroit for otolaryngology-head and neck surgery.7 They reported that females and patients who preferred provider-organization insurance were more likely to have a successful virtual visit than a telephone visit. They also found that increasing age and being in the lowest median household income quartile were associated with lower odds of completing a virtual visit. Dr Tam and her team, also at Henry Ford Hospital, working with head and neck cancer patients, found the same social determinants, which led to reduced success with video visits that did not cross over to telephone visits, highlighting a potential avenue for the continued care of cancer patients.8
Our pre-pandemic data showed the same top three counties receiving genetics care during the pandemic via telehealth despite differences in poverty level and income as outlined (Table 1 and Table 2). This is likely because of the multiple points of contact with the geneticist and genetics assistant through the first outreach phone call to make the appointment, a follow-up call to ensure they received their DNA collection kit, the genetics appointment when they learned how to do the self-saliva collection kit, then through a call letting them know a FedEx pickup had been scheduled, and finally, a results appointment. Because of multiple points of contact, this likely contributed to increased patient engagement and success with telehealth at our community program.
We appreciate that cancer genetic counseling is a unique discipline because the visits follow a format of a verbal review of the patient personal cancer history, family history of members with cancer, and counseling on background information on genes and their impact on cancer care. This format contributed well to either video or telephone visits, and the genetic testing companies that facilitated sending DNA collection kits to patients enabled us to coordinate genetics cancer care. Another factor that contributed to the success of our community hospital was that the community hospital provided Google Voice numbers at the beginning of the pandemic (Table 3).
This allowed patients to call the genetics assistant’s computer and immediately connect with her or call the geneticist versus being tied to an automated phone tree. Patients felt secure in contacting the department to inform the team when the DNA collection kit was ready for pickup.
The protocol for the genetics department was to send a saliva kit to the patient, so they had it on hand for the visit, and the geneticist could walk them through the collection, which significantly contributed to high success rates for this patient population. After collections were complete, patients could call the Google Number to schedule a FedEx pickup, and then they simply placed the packages on their doorstep.
Upon the completion of testing, patients would be called approximately 2 weeks later with their results. Google Voice allowed patients to feel connected to the genetics team, and if messages were left they were promptly returned, which contributed to patient engagement with their cancer genetics experience. Anecdotally, that engagement was reflected in fewer appointment no-shows and patients presenting for their results appointments to discuss how the genetic results would impact their care and that of their families.
While there was much success in offering telemedicine visits, there were some barriers that needed troubleshooting. Most patients took the appointments from the comfort of their homes, but some patients attempted to do their telehealth visits in public areas or while driving. In such instances, the geneticist offered to call the patients back at another more suitable time citing privacy or safety. Patients complied with this request. Other barriers included patients who had limited internet connectivity, those who did not have a smartphone, and patients who needed a translator or were hard of hearing. For these, accommodations had to be made.9,10,11
Conclusions
As the pandemic progressed, our genetics team adapted to a new normal and learned how to better provide virtual care to patients all over the state of Michigan. By proactively contacting patients and sending out kits prior to each virtual visit, our team was able to troubleshoot technical difficulties and could demonstrate how to label/self-collect a saliva sample while on the visit with our resident geneticist.
Patients from Detroit were as engaged and had similar visits as patients from surrounding zip codes. The data gathered from patients located in the surrounding Detroit zip codes contradicts the expected inequities associated with an urban setting. And while our community hospital program is small with one geneticist and one genetics coordinator, the lessons learned from this experience with telemedicine may help other programs with more resources and expand the way genetics can be utilized in the future.
Contributors
All authors provided substantial contributions to the design, analysis, interpretation of the data, and drafting of the manuscript. All authors approved and are accountable for all aspects of the work.
Acknowledgments
The authors thank Justin Beatty for his conscientious review of the manuscript, help with figures, and formatting, and editing, and Dr Susan Szpunar for her thoughtful input.
References
- Bach T. Why coronavirus is a disaster for Detroit [Internet]. 2020. Available from: https://www.usnews.com/news/cities/articles/2020-04-08/why-coronavirus-is-a-disaster-for-detroit [cited 28 November 2022].
- Poorest Cities in America 2023. World Population Review. 2023. Available from: https://worldpopulationreview.com/us-city-rankings/poorest-cities-in-america [cited 28 November 2022].
- Cuellar A, Pomeroy JML, Burla S, Jena AB. Outpatient care among users and nonusers of direct-to-patient telehealth: Observational study. J Med Internet Res. 2022;24(6):e37574. doi: 10.2196/37574
- Nouri S, Khoong E, Lyles CR, Karliner L. Addressing equity in telemedicine for chronic disease management during the COVID-19 pandemic. NEJM Catalyst. 2020. doi: 10.1056/CAT.20.012
- Jolie A. My medical choice. The New York Times, May 14, 2013.
- Thronson LR, Jackson SL, Chew LD. The pandemic of health care inequity. JAMA Netw Open. 2020;3(10):e2021767. doi: 10.1001/jamanetworkopen.2020.21767
- Darrat I, Tam S, Boulis M, Williams AM. Socioeconomic disparities in patient use of telehealth during the coronavirus disease 2019 surge. JAMA Otolaryngol Head Neck Surg. 2021;147(3):287. doi: 10.1001/jamaoto.2020.5161
- Tam S, Wu VF, Williams AM, Girgis M, Sheqwara JZ, Siddiqui F, et al. Disparities in the uptake of telemedicine during the COVID-19 surge in a multidisciplinary head and neck cancer population by patient demographic characteristics and socioeconomic status. JAMA Otolaryngol Head Neck Surg. 2021 Feb 1;147(2):209–11. doi: 10.1001/jamaoto.2020.3052
- Zoran S, Turcott C, Whitehead A, Hrabik L, Harris A, Schwoerer JS. Rapid transition to telemedicine during the COVID-19 pandemic: medical genetics experience. WMJ. 2021;120(3):218–21.
- Uhlmann WR, McKeon AJ, Wang C. Genetic counseling, virtual visits, and equity in the era of COVID-19 and beyond. J Genet Couns. 2021;30(4):1038–45. doi: 10.1002/jgc4.1469
- Mauer C, Zimmerman J, Lahiri S, Watson E, Parsi L, Berg J, et al. Adapting genetic counseling operations amidst the COVID-19 pandemic. J Genet Couns. 2021;30(4):949–55. doi: 10.1002/jgc4.1474
Copyright Ownership: This is an open-access article distributed in accordance with the Creative Commons Attribution Non-Commercial (CC BY-NC 4.0) license, which permits others to distribute, adapt, enhance this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0.